

Pepinemab antibody blockade of SEMA4D in early Huntington's disease: a randomized, placebo-controlled, phase 2 trial
- PMID: 35941373
- PMCID: PMC9361919
- DOI: 10.1038/s41591-022-01919-8
Pepinemab antibody blockade of SEMA4D in early Huntington's disease: a randomized, placebo-controlled, phase 2 trial
Erratum in
-
Publisher Correction: Pepinemab antibody blockade of SEMA4D in early Huntington's disease: a randomized, placebo-controlled, phase 2 trial.Nat Med. 2024 Feb;30(2):606. doi: 10.1038/s41591-022-02070-0. Nat Med. 2024. PMID: 36195687 Free PMC article. No abstract available.
Abstract
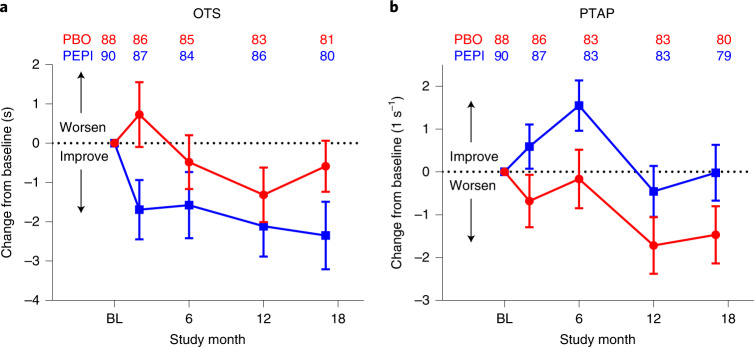
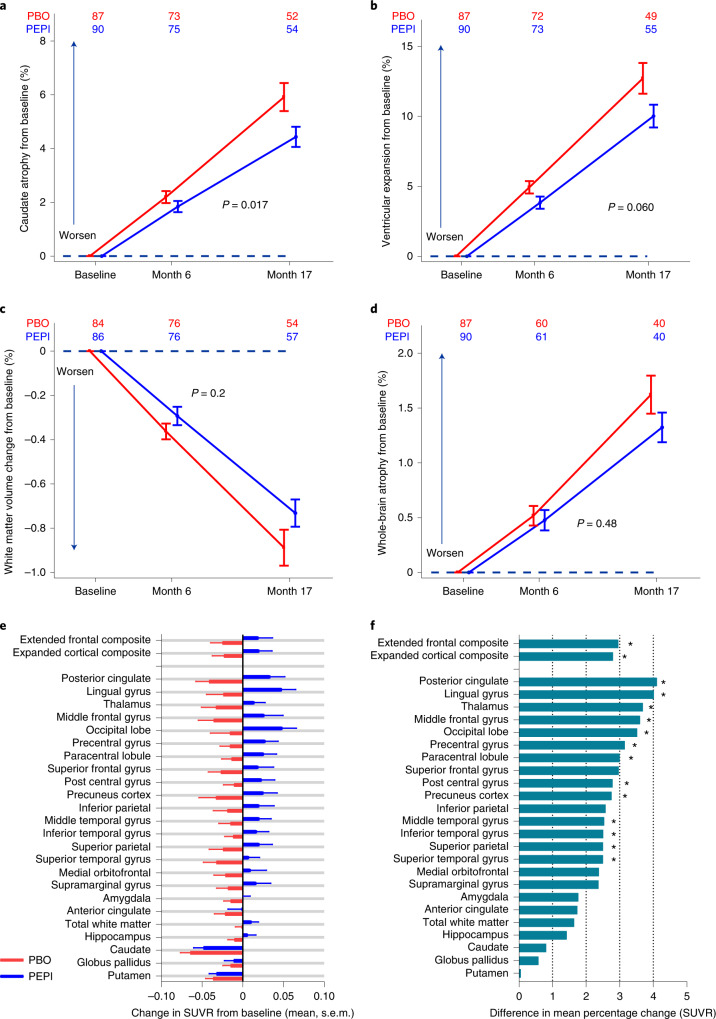
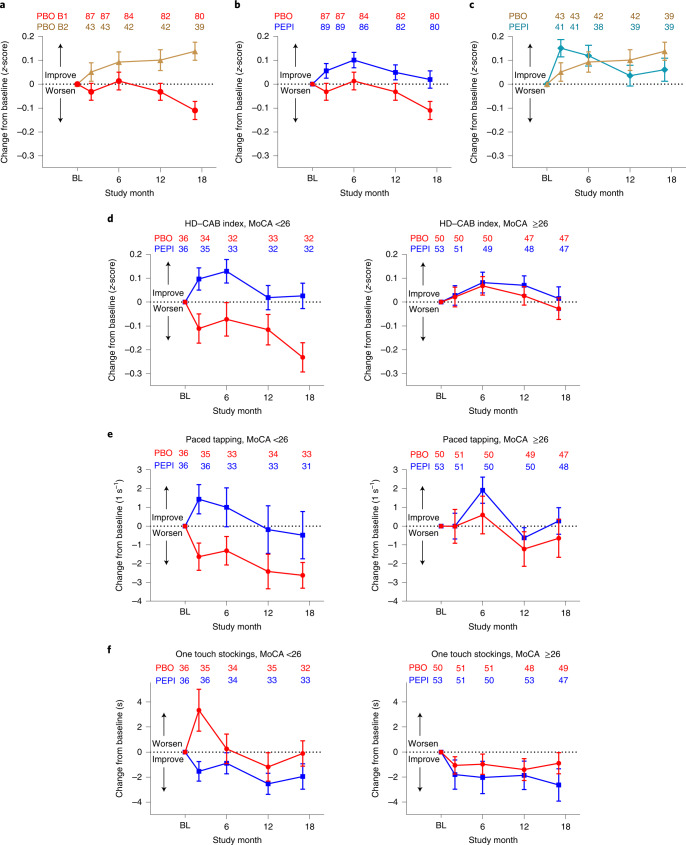
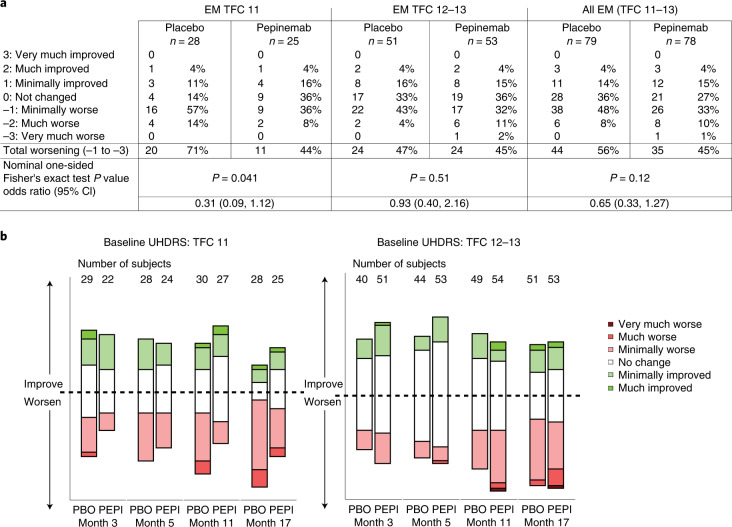
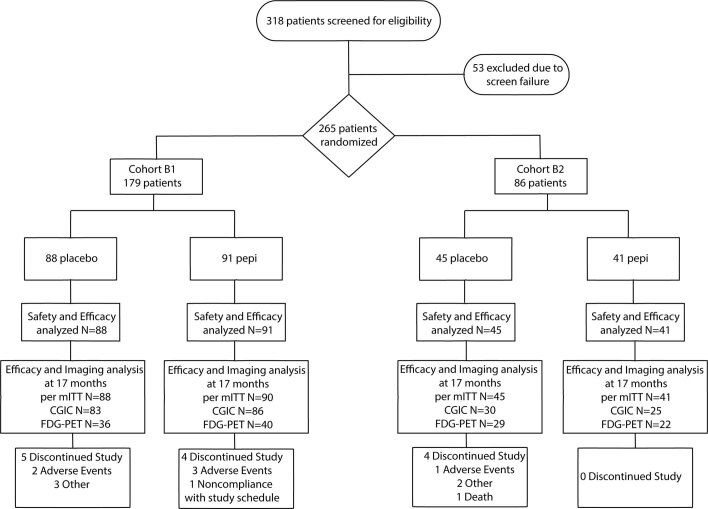
SIGNAL is a multicenter, randomized, double-blind, placebo-controlled phase 2 study (no. NCT02481674) established to evaluate pepinemab, a semaphorin 4D (SEMA4D)-blocking antibody, for treatment of Huntington's disease (HD). The trial enrolled a total of 265 HD gene expansion carriers with either early manifest (EM, n = 179) or late prodromal (LP, n = 86) HD, randomized (1:1) to receive 18 monthly infusions of pepinemab (n = 91 EM, 41 LP) or placebo (n = 88 EM, 45 LP). Pepinemab was generally well tolerated, with a relatively low frequency of serious treatment-emergent adverse events of 5% with pepinemab compared to 9% with placebo, including both EM and LP participants. Coprimary efficacy outcome measures consisted of assessments within the EM cohort of (1) a two-item HD cognitive assessment family comprising one-touch stockings of Cambridge (OTS) and paced tapping (PTAP) and (2) clinical global impression of change (CGIC). The differences between pepinemab and placebo in mean change (95% confidence interval) from baseline at month 17 for OTS were -1.98 (-4.00, 0.05) (one-sided P = 0.028), and for PTAP 1.43 (-0.37, 3.23) (one-sided P = 0.06). Similarly, because a significant treatment effect was not observed for CGIC, the coprimary endpoint, the study did not meet its prespecified primary outcomes. Nevertheless, a number of other positive outcomes and post hoc subgroup analyses-including additional cognitive measures and volumetric magnetic resonance imaging and fluorodeoxyglucose-positron-emission tomography imaging assessments-provide rationale and direction for the design of a phase 3 study and encourage the continued development of pepinemab in patients diagnosed with EM HD.
© 2022. The Author(s).
Conflict of interest statement
Vaccinex employment and stock: E.E.E., T.L.F., J.E.L., E.S., V.M. and M.Z. Vaccinex patents and applications related to SEMA4D (USPTO nos. 8,816,058, 9,090,709, 10,800,853 and 7,919,594): E.E.E., T.L.F., E.S. and M.Z. IXICO employment and stock: R.M. Research grant support from HSG, Neurocrine, Uniqure and Vaccinex: P.D. Payments to Clintrex Research Corporation for provision of research services during the conduct of the trial: K.D.K. Research funding from Vaccinex, CHDI, HDSA, Roche/Genentech, UniQure, HSG/NBI and Cures within Reach, consulting role for Teva and on Speaker’s Bureau of Sunovion Pharmaceuticals: E.F.S. Consultation fees from Amylyz, Novartis, Sage, Teva and Uniqure, grant funding from uniQure, Roche/Genentech, Triplet Therapeutics and CHDI and salary support from HSG for serving as chair of DSMB of a study funded by Neurocrine and the virtual UHDRS study: S. Frank. The remaining authors declare no competing interests.
Figures
References
-
- Glidden, A. et al. in Movement Disorders Vol. 32 (ed A. Jon Stoessl), Supplement 2, S183 (Wiley, 2017).
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
