

Stenting of the artery of Dr A.N. Kazantsev in the acute period of ischemic stroke
- PMID: 35942267
- PMCID: PMC9356102
- DOI: 10.1016/j.radcr.2022.07.034
Stenting of the artery of Dr A.N. Kazantsev in the acute period of ischemic stroke
Abstract
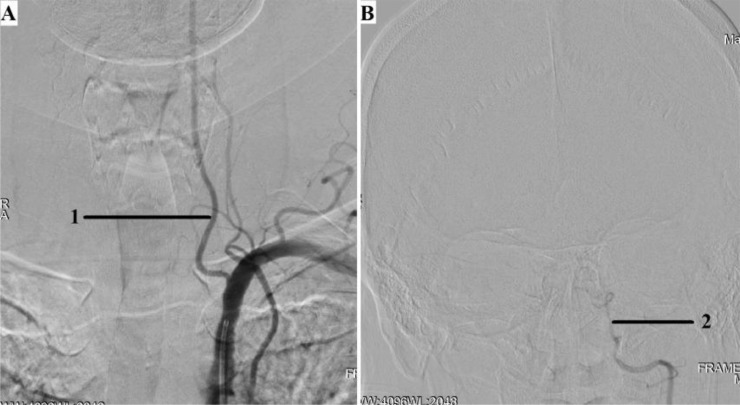
The A.N. Kazantsev artery is a vessel starting from the common carotid artery with subsequent bifurcation into 2 vessels of equal size-the internal carotid artery (ICA) and the persistent embryonic hypoglossal artery (PEHA). Until now, this artery has been considered as the ICA. However, according to all existing classifications, the ICA in the cervical segment does not have arterial branches. In addition, in view of the comparable sizes of PEHA and ICA, PEHA itself cannot be considered a branch of the ICA. Thus, by the right of the first description, the authors of the article named this vascular formation as the A.N. Kazantsev artery, which forms a bifurcation of the PEHA and ICA. In this clinical case, carotid angioplasty (CAS) was performed with stenting of 80% stenosis of the A.N. Kazantsev artery in the most acute period of acute cerebrovascular accident (ACV). According to angiography, the following was also revealed: the presence of PEHA, extending from the A.N. Kazantsev artery 5 cm above its mouth, connecting with the main artery; stenosis of the right vertebral artery 60% at the mouth; hypoplastic left vertebral artery with aplasia of the V4 segment; open circle of Willis (VC): absence of both posterior communicating arteries (PCA). Due to the high risk of recurrent CVA due to clamping of the A.N. Kazantsev artery during CEA, a multidisciplinary consultation decided to implement an emergency CAS of the A.N. Kazantsev artery. The distal embolism protection system FilterWire was inserted into the proximal part of the basilar artery through the radial artery on the left. The distal embolism protection system RX Accunet was inserted into the distal parts of the left ICA through the left common femoral artery. According to Seldinger, an Acculink stent 7-10 × 30 mm was inserted into the affected area of the A.N. Kazantsev artery, positioned and opened. The postoperative period was uneventful. ACV did not recur. Conducted dual antiplatelet therapy (acetylsalicylic acid 125 mg in the afternoon + clopidogrel 75 mg in the morning). The patient was discharged from the institution on the 10th day after the operation in a satisfactory condition.
Keywords: A.N. Kazantsev artery; Acute period of stroke; Carotid angioplasty with stenting; Carotid endarterectomy; Persistent embryonic hypoglossal artery; Stenting of the internal carotid artery.
© 2022 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures





References
-
- Altman D.A., Fokin A.A., Vladimirsky V.V., Baryshnikov A.A., Ignatov V.A., Chernousov V.V., et al. Immediate results of reconstructive interventions on the carotid arteries in patients in the acute stage of ischemic stroke. Bull Chelyabinsk Region Clin Hosp. 2018;2(40):40–44.
-
- Tsukurova L.A., Timchenko L.V., Golovko E.N., Usachev A.A., Fedorchenko A.N., Porkhanov V.A. Successful emergency surgical interventions on the brachiocephalic arteries in two patients in the acute period of ischemic stroke. Neurosurgery. 2013;(4):70–72.
-
- Dudanov I.P., Belinskaya V.G., Laptev K.V., Vasilchenko N.O., Koblov E.S., Sterlin O.V. Reconstructive surgery on the carotid arteries in the complex treatment of acute ischemic stroke. Med Acad J. 2011;11(2):109–116.
-
- Kazantsev A.N., Vinogradov R.A., Chernyavsky M.A., Kravchuk V.N., Matusevich V.V., Chernykh K.P., et al. Multicenter study: carotid endarterectomy in the first hours after ischemic stroke. Rus J Cardiol. 2021;26(6):76–80. doi: 10.15829/1560-4071-2021-4316. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
