

Non-timely clinically applicable ADC ratio in prostate mpMRI: a comparison with fusion biopsy results
- PMID: 35943517
- PMCID: PMC9560938
- DOI: 10.1007/s00261-022-03627-w
Non-timely clinically applicable ADC ratio in prostate mpMRI: a comparison with fusion biopsy results
Abstract
Purpose: The purpose of the study was to assess the diagnostic accuracy of ADC ratio and to evaluate its efficacy in reducing the number of false positives in prostatic mpMRI.
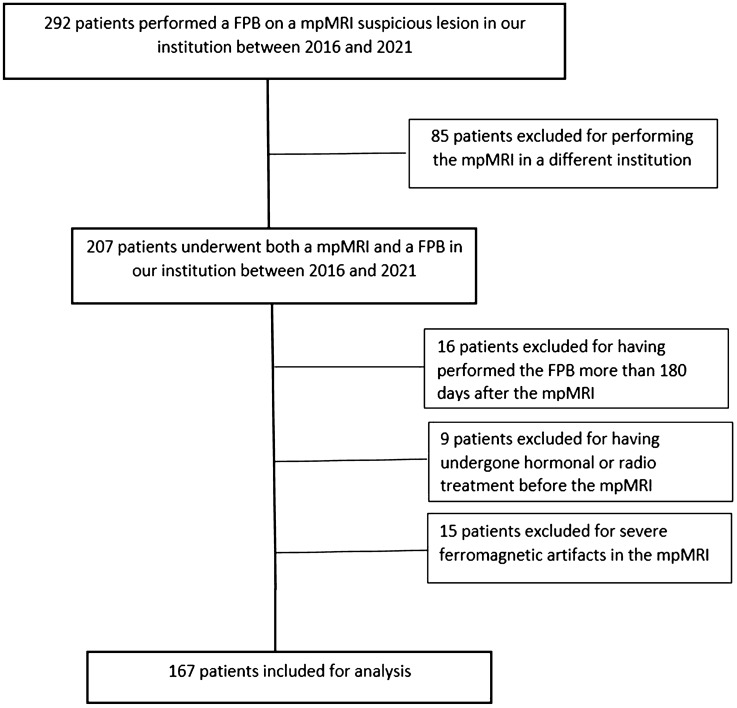
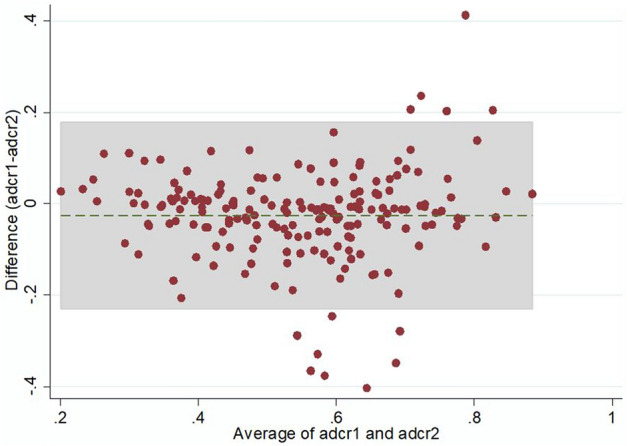
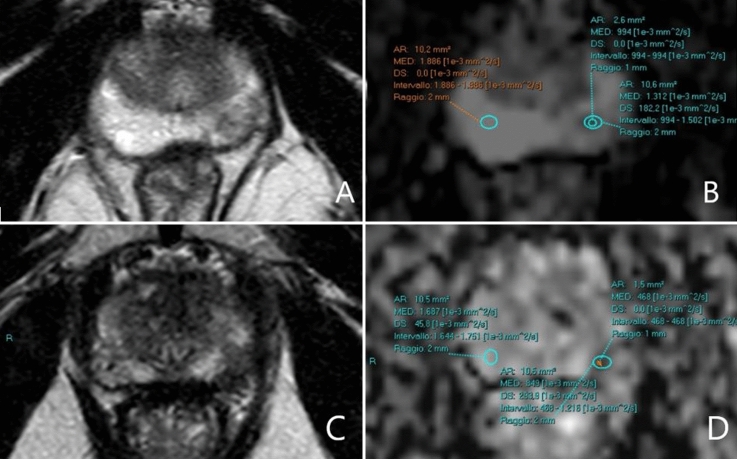
Materials and methods: All patients who underwent an mpMRI and a targeted fusion biopsy in our institution from 2016 to 2021 were retrospectively selected. Two experienced readers (R1 and R2) independently evaluated the images, blindly to biopsy results. The radiologists assessed the ADC ratios by tracing a circular 10 mm2 ROI on the biopsied lesion and on the apparently benign contralateral parenchyma. Prostate cancers were divided into non-clinically significant (nsPC, Gleason score = 6) and clinically significant (sPC, Gleason score ≥ 7). ROC analyses were performed.
Results: 167 patients and188 lesions were included. Concordance was 0.62 according to Cohen's K. ADC ratio showed an AUC for PCAs of 0.78 in R1 and 0.8 in R2. The AUC for sPC was 0.85 in R1 and 0.84 in R2. The 100% sensitivity cut-off for sPCs was 0.65 (specificity 25.6%) in R1 and 0.66 (specificity 27.4%) in R2. Forty-three benign or not clinically significant lesions were above the 0.65 threshold in R1; 46 were above the 0.66 cut-off in R2. This would have allowed to avoid an equal number of unnecessary biopsies at the cost of 2 nsPCs in R1 and one nsPC in R2.
Conclusion: In our sample, the ADC ratio was a useful and accurate tool that could potentially reduce the number of false positives in mpMRI.
Keywords: Apparent diffusion coefficient; Gleason score; Multiparametric MRI; Prostate cancer.
© 2022. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures


References
-
- Turkbey B, Rosenkrantz AB, Haider MA, Padhani AR, Villeirs G, Macura KJ, Tempany CM, Choyke PL, Cornud F, Margolis DJ, Thoeny HC, Verma S, Barentsz J, Weinreb JC. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur Urol. 2019;76(3):340–351. doi: 10.1016/j.eururo.2019.02.033. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
