

Effect of a Peer-Led Behavioral Intervention for Emergency Department Patients at High Risk of Fatal Opioid Overdose: A Randomized Clinical Trial
- PMID: 35943744
- PMCID: PMC9364125
- DOI: 10.1001/jamanetworkopen.2022.25582
Effect of a Peer-Led Behavioral Intervention for Emergency Department Patients at High Risk of Fatal Opioid Overdose: A Randomized Clinical Trial
Abstract
Importance: Fatal and nonfatal opioid overdoses are at record levels, and emergency department (ED) visits may be an opportune time to intervene. Peer-led models of care are increasingly common; however, little is known about their effectiveness.
Objective: To evaluate the effect of a peer-led behavioral intervention compared with the standard behavioral intervention delivered in the ED on engagement in substance use disorder (SUD) treatment within 30 days after the ED encounter.
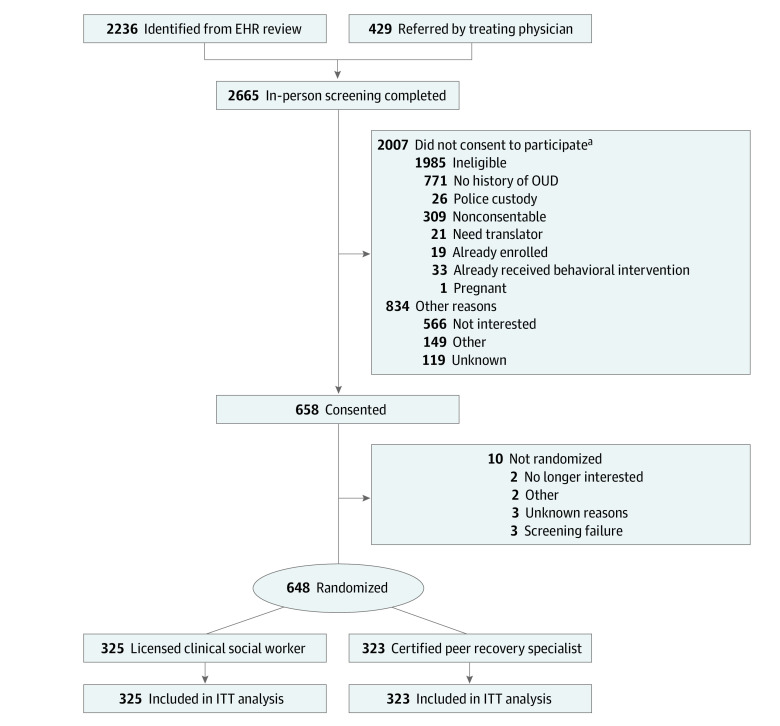
Design, setting, and participants: This randomized clinical trial recruited 648 patients from 2 EDs from November 15, 2018, to May 31, 2021. Patients were eligible to participate if they were in the ED for an opioid overdose, receiving treatment related to an opioid use disorder, or identified as having had a recent opioid overdose.
Interventions: Participants were randomly assigned to receive a behavioral intervention from a certified peer recovery specialist (n = 323) or a standard intervention delivered by a hospital-employed licensed clinical social worker (n = 325). A certified peer recovery specialist was someone with at least 2 years of recovery who completed a 45-hour training program and had 500 hours of supervised work experience. After the ED intervention, the certified peer recovery specialists offered continued contact with participants for up to 90 days.
Main outcomes and measures: The primary outcome was receipt of SUD treatment within 30 days of enrollment, assessed with deterministic linkage of statewide administrative databases. Treatment engagement was defined as admission to a formal, publicly licensed SUD treatment program or receipt of office-based medication for opioid use disorder within 30 days of the initial ED visit.
Results: Among the 648 participants, the mean (SD) age was 36.9 (10.8) years, and most were male (442 [68.2%]) and White (444 [68.5%]). Receipt of SUD treatment occurred for 103 of 323 participants (32%) in the intervention group vs 98 of 325 participants (30%) in the usual care group within 30 days of the ED visit. Among all participants, the most accessed treatments were outpatient medication for opioid use disorder (buprenorphine, 119 [18.4%]; methadone, 44 [6.8%]) and residential treatment (44 [6.8%]).
Conclusions and relevance: Overall, this study found that a substantial proportion of participants in both groups engaged in SUD treatment within 30 days of the ED visit. An ED-based behavioral intervention is likely effective in promoting treatment engagement, but who delivers the intervention may be less influential on short-term outcomes. Further study is required to determine the effects on longer-term engagement in SUD care and other health outcomes (eg, recurrent overdose).
Trial registration: ClinicalTrials.gov Identifier: NCT03684681.
Conflict of interest statement
Figures
References
-
- National Institute on Drug Abuse . Overdose death rates. National Institutes of Health. Published January 20, 2022. Accessed March 3, 2022. https://nida.nih.gov/drug-topics/trends-statistics/overdose-death-rates
-
- Drug overdose deaths in the US: top 100,000 annually. News release. National Center for Health Statistics, Centers for Disease Control and Prevention. November 17, 2021. Accessed March 29, 2022. https://www.cdc.gov/nchs/pressroom/nchs_press_releases/2021/20211117.htm
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
