

Predicting Mortality in Intensive Care Unit Patients With Heart Failure Using an Interpretable Machine Learning Model: Retrospective Cohort Study
- PMID: 35943767
- PMCID: PMC9399880
- DOI: 10.2196/38082
Predicting Mortality in Intensive Care Unit Patients With Heart Failure Using an Interpretable Machine Learning Model: Retrospective Cohort Study
Abstract
Background: Heart failure (HF) is a common disease and a major public health problem. HF mortality prediction is critical for developing individualized prevention and treatment plans. However, due to their lack of interpretability, most HF mortality prediction models have not yet reached clinical practice.
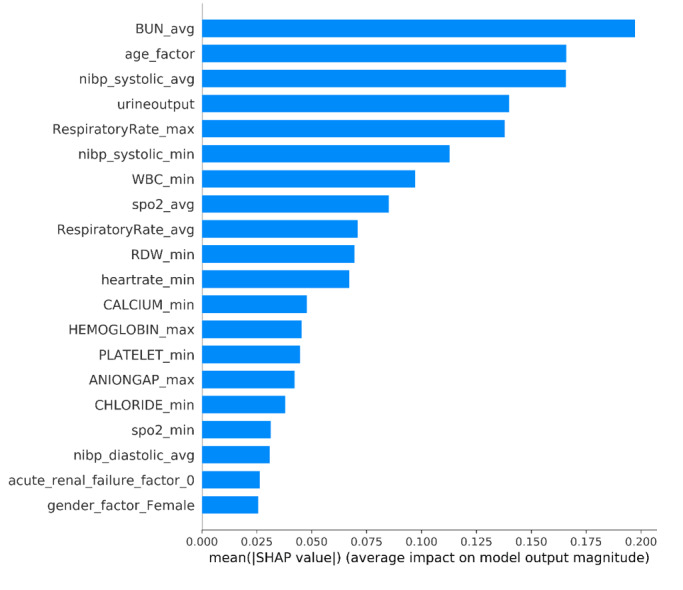
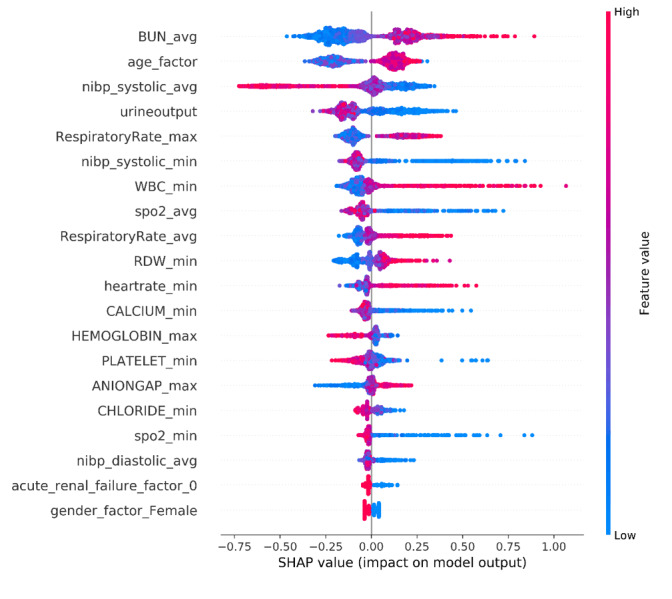
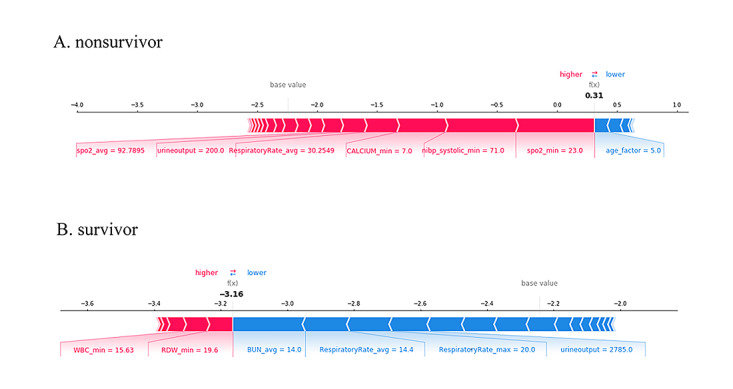
Objective: We aimed to develop an interpretable model to predict the mortality risk for patients with HF in intensive care units (ICUs) and used the SHapley Additive exPlanation (SHAP) method to explain the extreme gradient boosting (XGBoost) model and explore prognostic factors for HF.
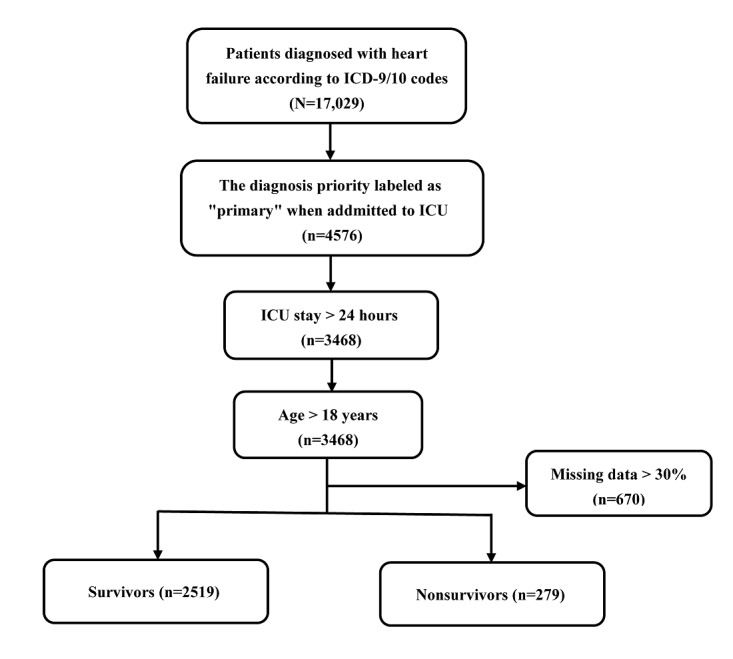
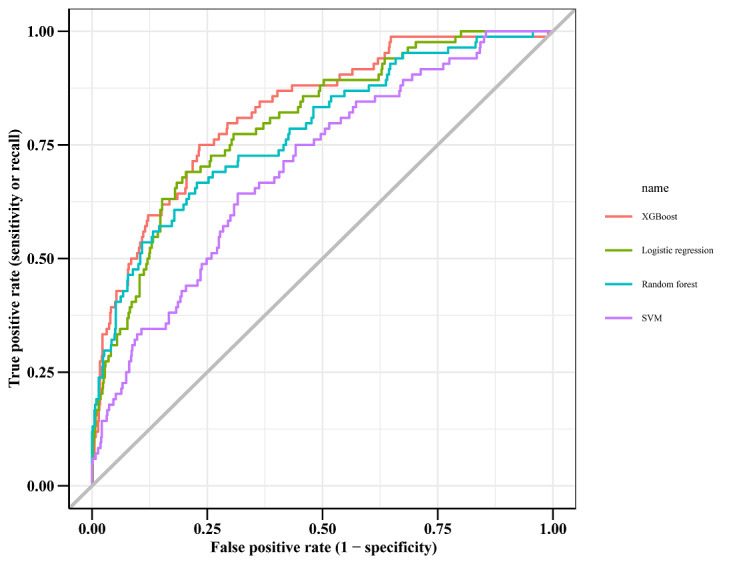
Methods: In this retrospective cohort study, we achieved model development and performance comparison on the eICU Collaborative Research Database (eICU-CRD). We extracted data during the first 24 hours of each ICU admission, and the data set was randomly divided, with 70% used for model training and 30% used for model validation. The prediction performance of the XGBoost model was compared with three other machine learning models by the area under the curve. We used the SHAP method to explain the XGBoost model.
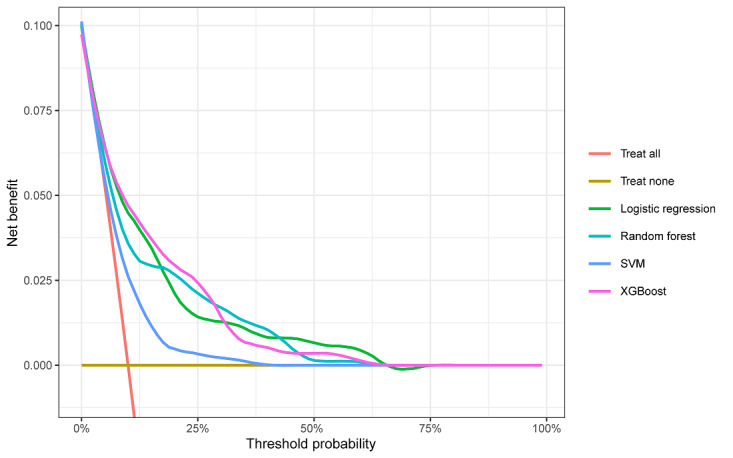
Results: A total of 2798 eligible patients with HF were included in the final cohort for this study. The observed in-hospital mortality of patients with HF was 9.97%. Comparatively, the XGBoost model had the highest predictive performance among four models with an area under the curve (AUC) of 0.824 (95% CI 0.7766-0.8708), whereas support vector machine had the poorest generalization ability (AUC=0.701, 95% CI 0.6433-0.7582). The decision curve showed that the net benefit of the XGBoost model surpassed those of other machine learning models at 10%~28% threshold probabilities. The SHAP method reveals the top 20 predictors of HF according to the importance ranking, and the average of the blood urea nitrogen was recognized as the most important predictor variable.
Conclusions: The interpretable predictive model helps physicians more accurately predict the mortality risk in ICU patients with HF, and therefore, provides better treatment plans and optimal resource allocation for their patients. In addition, the interpretable framework can increase the transparency of the model and facilitate understanding the reliability of the predictive model for the physicians.
Keywords: SHAP; SHapley Additive exPlanation; XGBoost; heart failure; intensive care unit; mortality; prediction.
©Jili Li, Siru Liu, Yundi Hu, Lingfeng Zhu, Yujia Mao, Jialin Liu. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 09.08.2022.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Ambrosy AP, Fonarow GC, Butler J, Chioncel O, Greene SJ, Vaduganathan M, Nodari S, Lam CSP, Sato N, Shah AN, Gheorghiade M. The global health and economic burden of hospitalizations for heart failure: lessons learned from hospitalized heart failure registries. J Am Coll Cardiol. 2014 Apr 1;63(12):1123–33. doi: 10.1016/j.jacc.2013.11.053. http://linkinghub.elsevier.com/retrieve/pii/S0735-1097(14)00291-5 S0735-1097(14)00291-5 - DOI - PubMed
-
- Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, Fonarow GC, Ikonomidis JS, Khavjou O, Konstam MA, Maddox TM, Nichol G, Pham M, Piña IL, Trogdon JG, American HAACC, Council OATB, Council OCR, Council OCC, Council OE, Stroke C. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013 May;6(3):606–19. doi: 10.1161/HHF.0b013e318291329a. http://circheartfailure.ahajournals.org/cgi/pmidlookup?view=long&pmid=23... HHF.0b013e318291329a - DOI - PMC - PubMed
-
- Liao L, Allen LA, Whellan DJ. Economic burden of heart failure in the elderly. Pharmacoeconomics. 2008;26(6):447–62.2661 - PubMed
-
- Kim HJ, Park M, Shin JI, Park J, Kim D, Jeon J, Kim J, Song T. Associations of heart failure with susceptibility and severe complications of COVID-19: a nationwide cohort study. J Med Virol. 2021 Nov 05;:1138–1145. doi: 10.1002/jmv.27435. http://europepmc.org/abstract/MED/34738248 - DOI - PMC - PubMed
-
- Yonas E, Alwi I, Pranata R, Huang I, Lim MA, Gutierrez EJ, Yamin M, Siswanto BB, Virani SS. Effect of heart failure on the outcome of COVID-19 - a meta analysis and systematic review. Am J Emerg Med. 2021 Aug;46:204–211. doi: 10.1016/j.ajem.2020.07.009. http://europepmc.org/abstract/MED/33071085 S0735-6757(20)30602-1 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
