

Genome-wide association studies of global Mycobacterium tuberculosis resistance to 13 antimicrobials in 10,228 genomes identify new resistance mechanisms
- PMID: 35944070
- PMCID: PMC9363015
- DOI: 10.1371/journal.pbio.3001755
Genome-wide association studies of global Mycobacterium tuberculosis resistance to 13 antimicrobials in 10,228 genomes identify new resistance mechanisms
Abstract
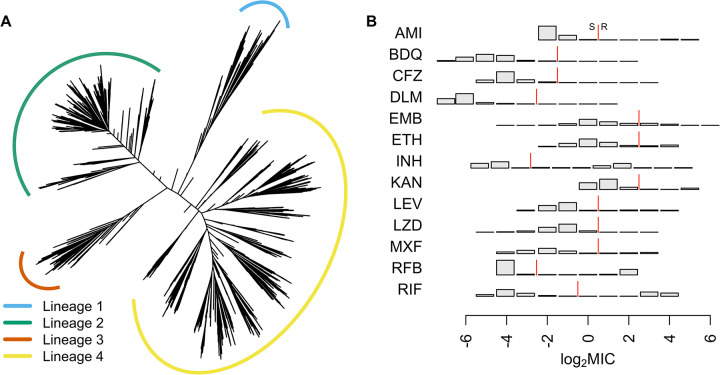
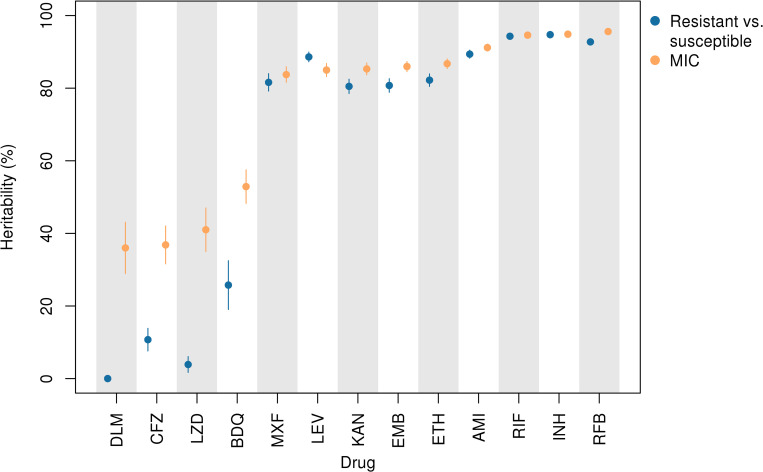
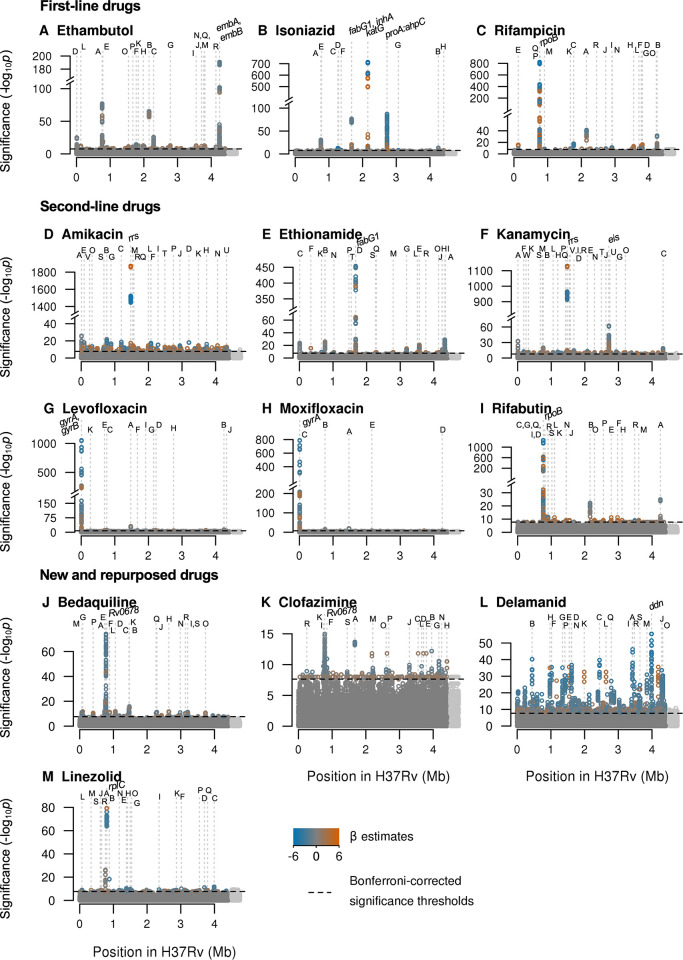
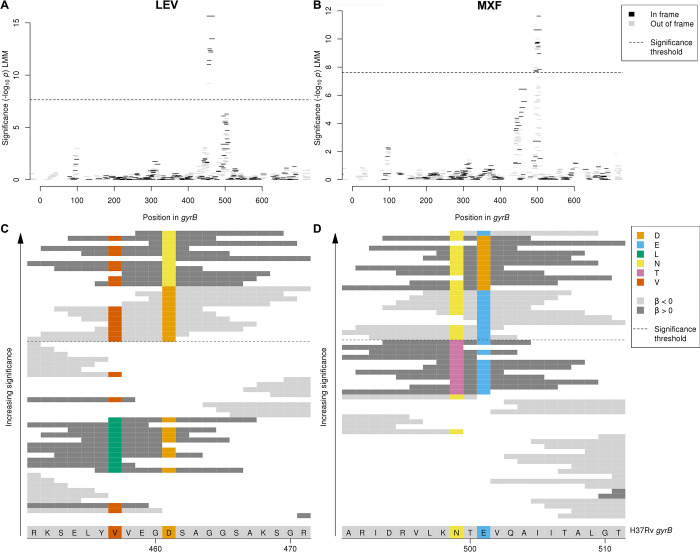
The emergence of drug-resistant tuberculosis is a major global public health concern that threatens the ability to control the disease. Whole-genome sequencing as a tool to rapidly diagnose resistant infections can transform patient treatment and clinical practice. While resistance mechanisms are well understood for some drugs, there are likely many mechanisms yet to be uncovered, particularly for new and repurposed drugs. We sequenced 10,228 Mycobacterium tuberculosis (MTB) isolates worldwide and determined the minimum inhibitory concentration (MIC) on a grid of 2-fold concentration dilutions for 13 antimicrobials using quantitative microtiter plate assays. We performed oligopeptide- and oligonucleotide-based genome-wide association studies using linear mixed models to discover resistance-conferring mechanisms not currently catalogued. Use of MIC over binary resistance phenotypes increased sample heritability for the new and repurposed drugs by 26% to 37%, increasing our ability to detect novel associations. For all drugs, we discovered uncatalogued variants associated with MIC, including in the Rv1218c promoter binding site of the transcriptional repressor Rv1219c (isoniazid), upstream of the vapBC20 operon that cleaves 23S rRNA (linezolid) and in the region encoding an α-helix lining the active site of Cyp142 (clofazimine, all p < 10-7.7). We observed that artefactual signals of cross-resistance could be unravelled based on the relative effect size on MIC. Our study demonstrates the ability of very large-scale studies to substantially improve our knowledge of genetic variants associated with antimicrobial resistance in M. tuberculosis.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: E.R. is employed by Public Health England and holds an honorary contract with Imperial College London. I.F.L. is Director of the Scottish Mycobacteria Reference Laboratory. S.N. receives funding from German Center for Infection Research, Excellenz Cluster Precision Medicine in Chronic Inflammation, Leibniz Science Campus Evolutionary Medicine of the LUNG (EvoLUNG)tion EXC 2167. P.S. is a consultant at Genoscreen. T.R. is funded by NIH and DoD and receives salary support from the non-profit organization FIND. T.R. is a co-founder, board member and shareholder of Verus Diagnostics Inc, a company that was founded with the intent of developing diagnostic assays. Verus Diagnostics was not involved in any way with data collection, analysis or publication of the results. T.R. has not received any financial support from Verus Diagnostics. UCSD Conflict of Interest office has reviewed and approved T.R.’s role in Verus Diagnostics Inc. T.R. is a co-inventor of a provisional patent for a TB diagnostic assay (provisional patent #: 63/048.989). T.R. is a co-inventor on a patent associated with the processing of TB sequencing data (European Patent Application No. 14840432.0 & USSN 14/912,918). T.R. has agreed to “donate all present and future interest in and rights to royalties from this patent” to UCSD to ensure that he does not receive any financial benefits from this patent. S.S. is working and holding ESOPs at HaystackAnalytics Pvt. Ltd. (Product: Using whole genome sequencing for drug susceptibility testing for Mycobacterium tuberculosis). G.F.G. is listed as an inventor on patent applications for RBD-dimer-based CoV vaccines. The patents for RBD-dimers as protein subunit vaccines for SARS-CoV-2 have been licensed to Anhui Zhifei Longcom Biopharmaceutical Co. Ltd, China.
Figures
References
-
- World Health Organization. Global Tuberculosis. Report 2020.
-
- World Health Organization. WHO Consolidated Guidelines on Tuberculosis, Module 4: Treatment -. Drug-Resistant Tuberculosis Treatment 2020. - PubMed
-
- World Health Organization. Rapid Communication: Key changes to the treatment of drug-resistant tuberculosis. 2019.
Publication types
MeSH terms
Substances
Grants and funding
- U60 OE000103/OE/OSELS CDC HHS/United States
- 214560/Z/18/Z/WT_/Wellcome Trust/United Kingdom
- T32 GM007365/GM/NIGMS NIH HHS/United States
- 203135/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- 098316 /WT_/Wellcome Trust/United Kingdom
- FC0010218/WT_/Wellcome Trust/United Kingdom
- 203919/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- 206724/Z/17/Z/WT_/Wellcome Trust/United Kingdom
- R01 AI146338/AI/NIAID NIH HHS/United States
- 201470/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- 101237/Z/13/B/WT_/Wellcome Trust/United Kingdom
- 200205/Z/15/Z/WT_/Wellcome Trust/United Kingdom
- 203583/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- 203141/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- DH_/Department of Health/United Kingdom
- 214321/Z/18/Z/WT_/Wellcome Trust/United Kingdom
- R03 AI117312/AI/NIAID NIH HHS/United States
- FC0010218/CRUK_/Cancer Research UK/United Kingdom
LinkOut - more resources
Full Text Sources
