

Peanut-Specific IgG4 and IgA in Saliva Are Modulated by Peanut Oral Immunotherapy
- PMID: 35944894
- PMCID: PMC9742136
- DOI: 10.1016/j.jaip.2022.07.030
Peanut-Specific IgG4 and IgA in Saliva Are Modulated by Peanut Oral Immunotherapy
Abstract
Background: Antigen-specific immunoglobulin responses have yet to be studied at the oral mucosal surface during peanut oral immunotherapy (PnOIT).
Objective: We aimed to quantify salivary peanut-specific IgG4 (PNsIgG4) and IgA (PNsIgA) and total IgG4 and IgA in participants from the Immune Tolerance Network's IMPACT study, a phase 2 PnOIT trial.
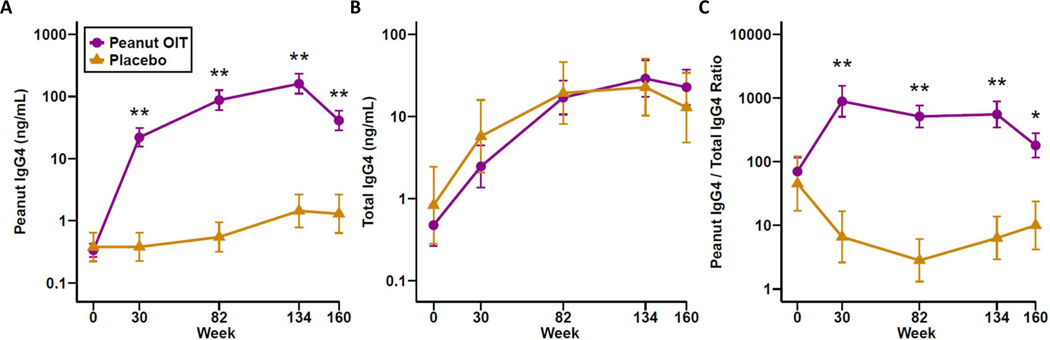
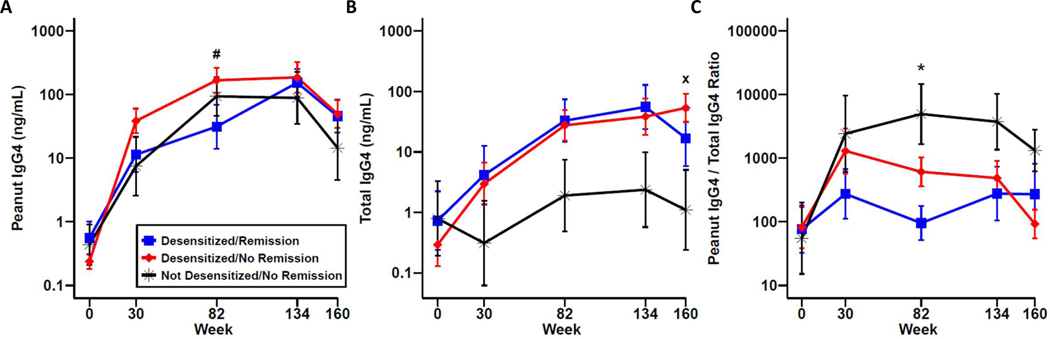
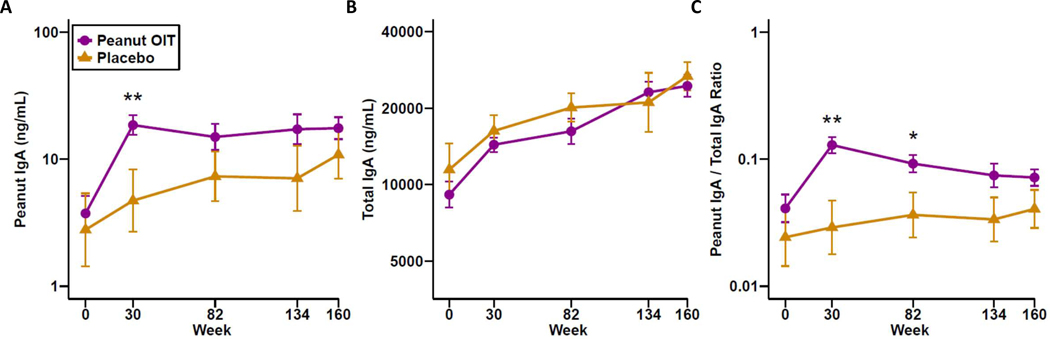
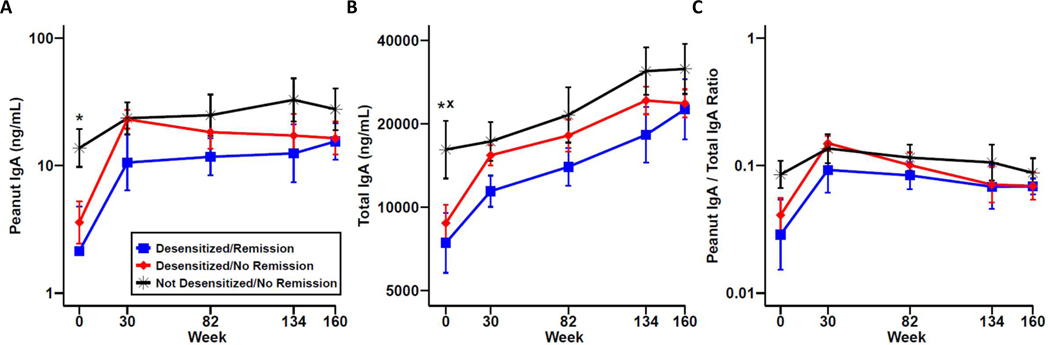
Methods: Peanut-allergic children, aged 12 months to younger than 48 months at screening, were enrolled and randomized to PnOIT or placebo oral immunotherapy (OIT) for 134 weeks. Per-protocol analysis included 69 PnOIT and 23 placebo participants. Double-blind, placebo-controlled food challenges were conducted at weeks 134 and 160 to assess desensitization and remission, respectively. Saliva samples were collected at baseline and 30, 82, 134, and 160 weeks to quantify PNsIgG4, PNsIgA, and total IgG4 and IgA.
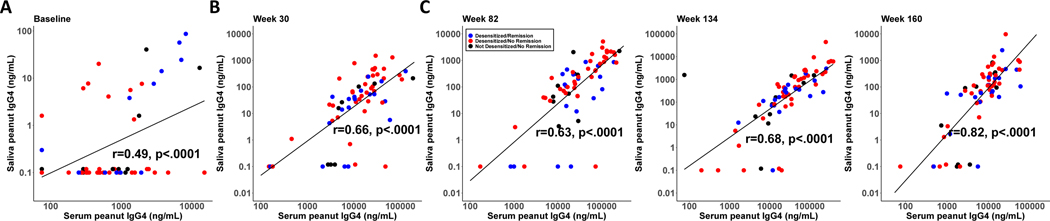
Results: Participants who received PnOIT experienced significant increases in PNsIgG4 in saliva, whereas participants on placebo did not (P < .01 at all time points). The PNsIgA/total IgA ratio was also significantly increased in participants treated with PnOIT when compared with those receiving placebo at 30 and 82 weeks (P < .05). During PnOIT, desensitized participants had increased PNsIgA that plateaued, whereas the not desensitized/no remission group did not change over time. Interestingly, when the PnOIT group was evaluated by clinical outcome, PNsIgA was higher at baseline in the not desensitized/no remission group than in the desensitized/remission group (P < .05).
Conclusions: PnOIT induces substantial increases in allergen-specific IgG4 and IgA in saliva. These data provide insight into OIT-induced mucosal responses and suggest the utility of these easily obtained samples for biomarker development.
Keywords: IgA; IgG4; Oral immunotherapy; Peanut allergy; Saliva.
Copyright © 2022 American Academy of Allergy, Asthma & Immunology. All rights reserved.
Figures
References
-
- Investigators PGoC, Vickery BP, Vereda A, Casale TB, Beyer K, du Toit G, et al. AR101 Oral Immunotherapy for Peanut Allergy. N Engl J Med. 2018;379(21):1991–2001. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
