

Transoral Robotic Surgery for Recurrent Tumors of the Upper Aerodigestive Tract (RECUT): An International Cohort Study
- PMID: 35944904
- PMCID: PMC9552281
- DOI: 10.1093/jnci/djac130
Transoral Robotic Surgery for Recurrent Tumors of the Upper Aerodigestive Tract (RECUT): An International Cohort Study
Abstract
Background: Transoral robotic surgery (TORS) is an emerging minimally invasive surgical treatment for residual, recurrent, and new primary head and neck cancers in previously irradiated fields, with limited evidence for its oncological effectiveness.
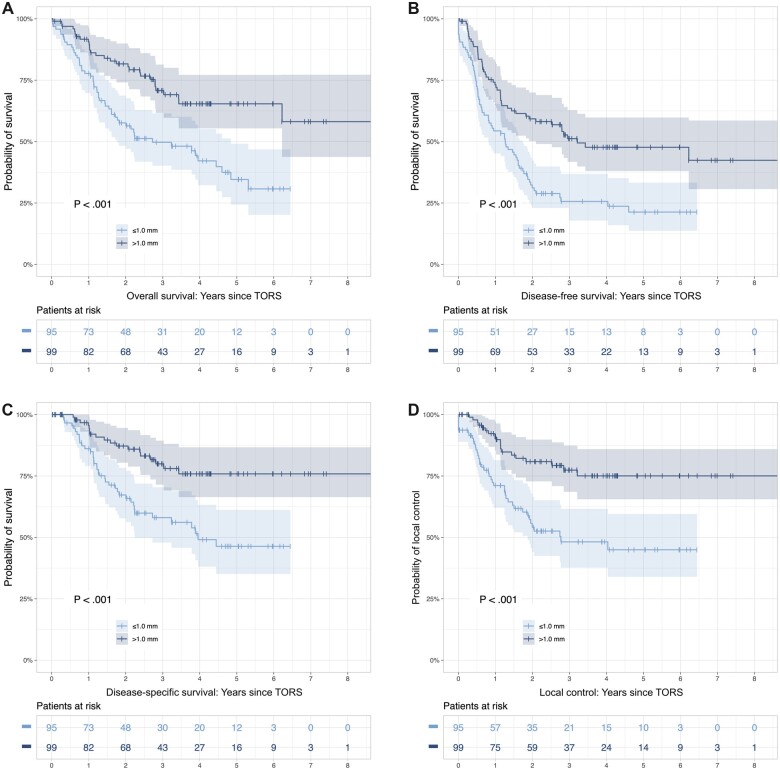
Methods: A retrospective observational cohort study of consecutive cases performed in 16 high-volume international centers before August 2018 was conducted (registered at clinicaltrials.gov [NCT04673929] as the RECUT study). Overall survival (OS), disease-free survival, disease-specific survivals (DSS), and local control (LC) were calculated using Kaplan-Meier estimates, with subgroups compared using log-rank tests and Cox proportional hazards modeling for multivariable analysis. Maximally selected rank statistics determined the cut point for closest surgical resection margin based on LC.
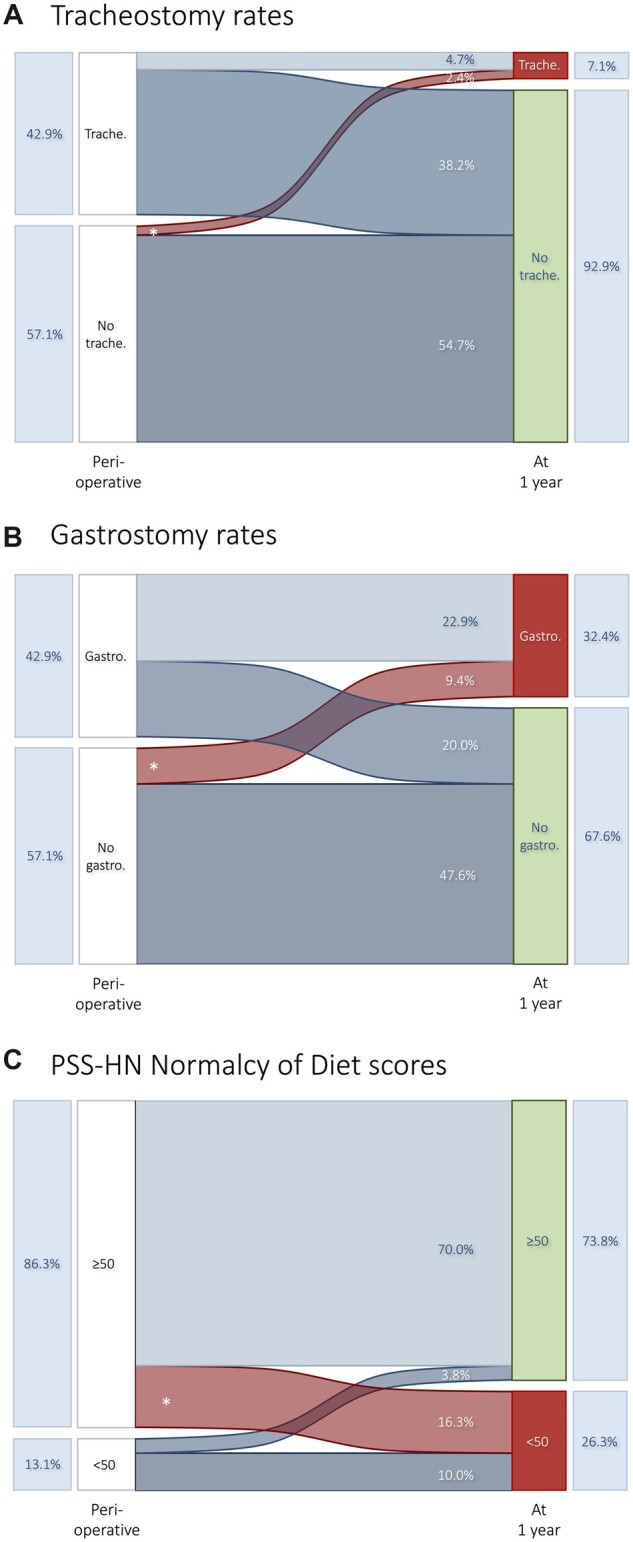
Results: Data for 278 eligible patients were analyzed, with median follow-up of 38.5 months. Two-year and 5-year outcomes were 69.0% and 62.2% for LC, 71.8% and 49.8% for OS, 47.2% and 35.7% for disease-free survival, and 78.7% and 59.1% for disease-specific survivals. The most discriminating margin cut point was 1.0 mm; the 2-year LC was 80.9% above and 54.2% below or equal to 1.0 mm. Increasing age, current smoking, primary tumor classification, and narrow surgical margins (≤1.0 mm) were statistically significantly associated with lower OS. Hemorrhage with return to theater was seen in 8.1% (n = 22 of 272), and 30-day mortality was 1.8% (n = 5 of 272). At 1 year, 10.8% (n = 21 of 195) used tracheostomies, 33.8% (n = 66 of 195) used gastrostomies, and 66.3% (n = 53 of 80) had maintained or improved normalcy of diet scores.
Conclusions: Data from international centers show TORS to treat head and neck cancers in previously irradiated fields yields favorable outcomes for LC and survival. Where feasible, TORS should be considered the preferred surgical treatment in the salvage setting.
© The Author(s) 2022. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures

References
-
- Brockstein B, Haraf DJ, Rademaker AW, et al. Patterns of failure, prognostic factors and survival in locoregionally advanced head and neck cancer treated with concomitant chemoradiotherapy: a 9-year, 337-patient, multi-institutional experience. Ann Oncol. 2004;15(8):1179-1186. doi: 10.1093/annonc/mdh308. - DOI - PubMed
