

Multicenter Analysis of Cardiometabolic-related Diagnoses in Transgender and Gender-Diverse Youth: A PEDSnet Study
- PMID: 35945152
- PMCID: PMC9516032
- DOI: 10.1210/clinem/dgac469
Multicenter Analysis of Cardiometabolic-related Diagnoses in Transgender and Gender-Diverse Youth: A PEDSnet Study
Abstract
Context: Studies on cardiometabolic health in transgender and gender-diverse youth (TGDY) are limited to small cohorts.
Objective: This work aimed to determine the odds of cardiometabolic-related diagnoses in TGDY compared to matched controls in a cross-sectional analysis, using a large, multisite database (PEDSnet).
Methods: Electronic health record data (2009-2019) were used to determine odds of cardiometabolic-related outcomes based on diagnosis, anthropometric, and laboratory data using logistic regression among TGDY youth vs controls. The association of gender-affirming hormone therapy (GAHT) with these outcomes was examined separately among TGDY. TGDY (n = 4172) were extracted from 6 PEDSnet sites and propensity-score matched on 8 variables to controls (n = 16 648). Main outcomes measures included odds of having cardiometabolic-related diagnoses among TGDY compared to matched controls, and among TGDY prescribed GAHT compared to those not prescribed GAHT.
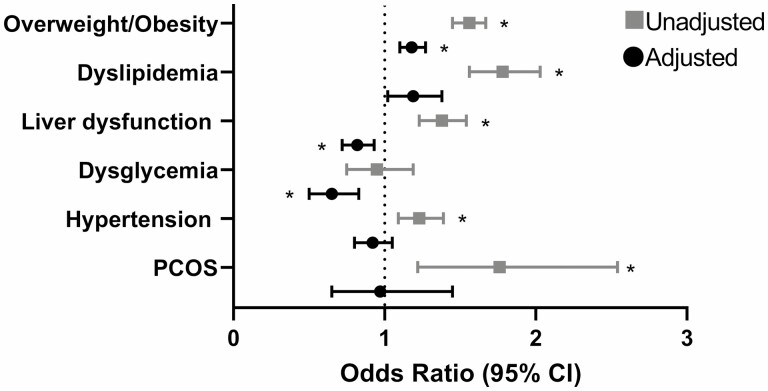
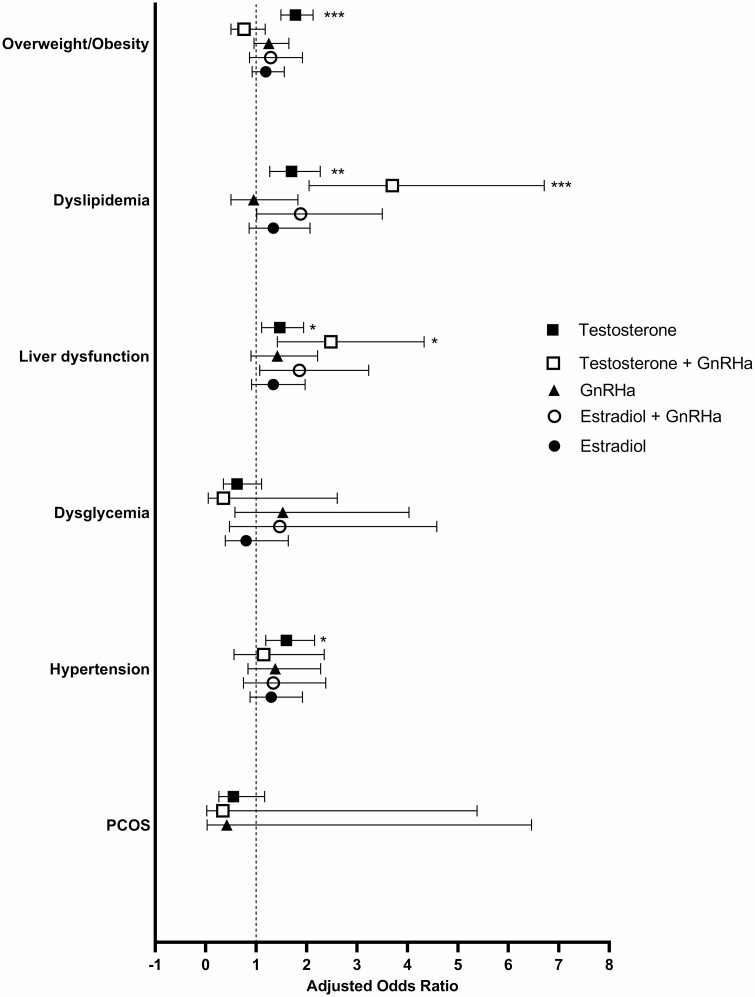
Results: In adjusted analyses, TGDY had higher odds of overweight/obesity (1.2; 95% CI, 1.1-1.3) than controls. TGDY with a testosterone prescription alone or in combination with a gonadotropin-releasing hormone agonist (GnRHa) had higher odds of dyslipidemia (1.7; 95% CI, 1.3-2.3 and 3.7; 95% CI, 2.1-6.7, respectively) and liver dysfunction (1.5; 95% CI, 1.1-1.9 and 2.5; 95% CI, 1.4-4.3) than TGDY not prescribed GAHT. TGDY with a testosterone prescription alone had higher odds of overweight/obesity (1.8; 95% CI, 1.5-2.1) and hypertension (1.6 95% CI, 1.2-2.2) than those not prescribed testosterone. Estradiol and GnRHa alone were not associated with greater odds of cardiometabolic-related diagnoses.
Conclusion: TGDY have increased odds of overweight/obesity compared to matched controls. Screening and tailored weight management, sensitive to the needs of TGDY, are needed.
Keywords: body mass index; cardiometabolic; cholesterol; gender dysphoria; hormone therapy; pediatric.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Endocrine Society. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Cardiometabolic Outcomes in Transgender Youth.J Clin Endocrinol Metab. 2022 Nov 25;107(12):e4380-e4381. doi: 10.1210/clinem/dgac592. J Clin Endocrinol Metab. 2022. PMID: 36221797 No abstract available.
References
-
- Johns MM, Lowry R, Andrzejewski J, et al. . Transgender identity and experiences of violence victimization, substance use, suicide risk, and sexual risk behaviors among high school students—19 states and large urban school districts, 2017. Morb Mortal Wkly Rep. 2019;68(3):67-71. doi:10.15585/mmwr.mm6803a3 - DOI - PMC - PubMed
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. 5th ed.American Psychiatric Association; 2013:xliv, 947.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
