

Genetic alterations of Keap1 confers chemotherapeutic resistance through functional activation of Nrf2 and Notch pathway in head and neck squamous cell carcinoma
- PMID: 35945195
- PMCID: PMC9363464
- DOI: 10.1038/s41419-022-05126-8
Genetic alterations of Keap1 confers chemotherapeutic resistance through functional activation of Nrf2 and Notch pathway in head and neck squamous cell carcinoma
Abstract
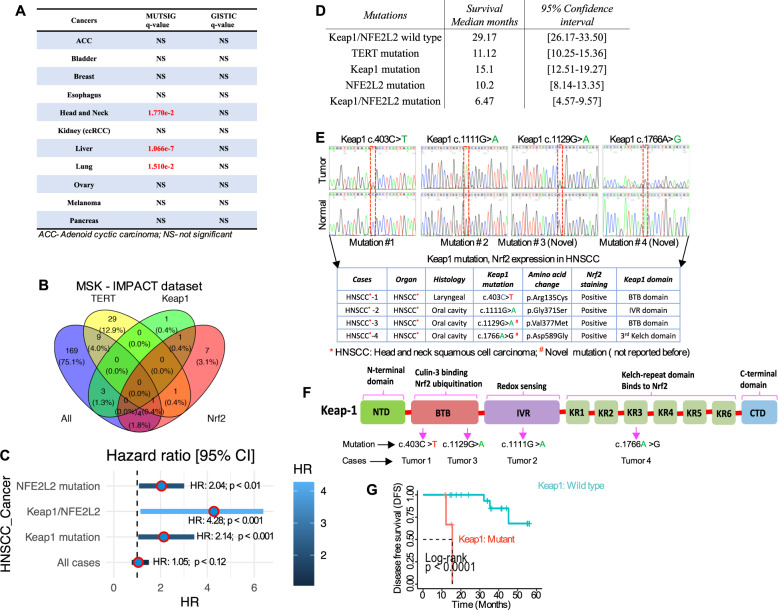
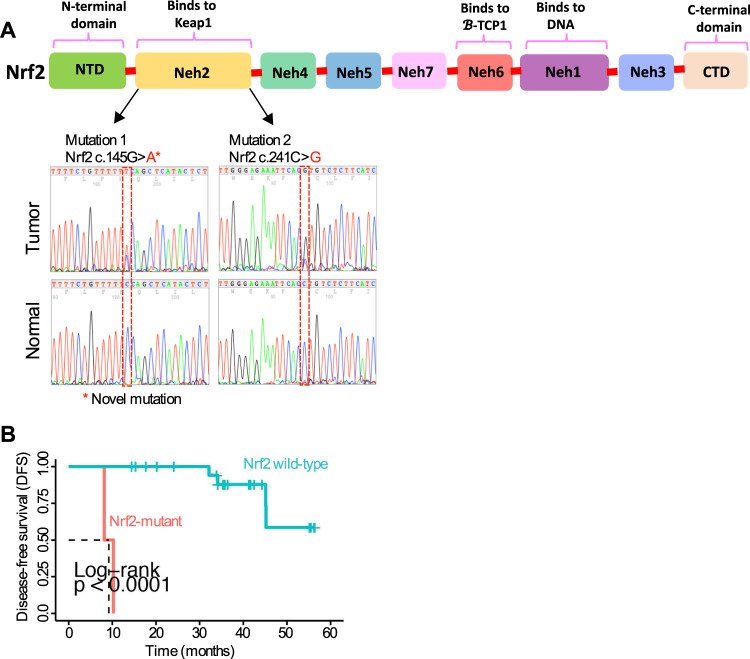
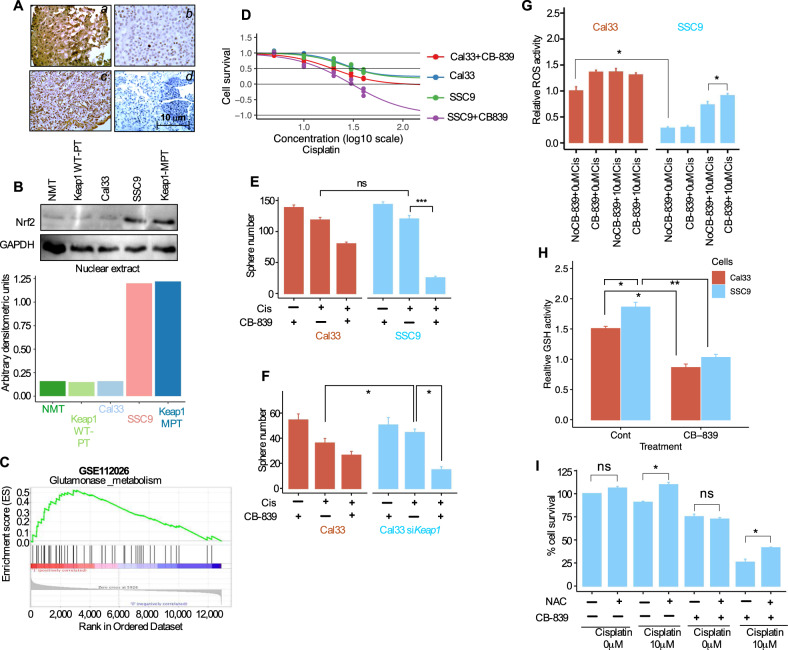
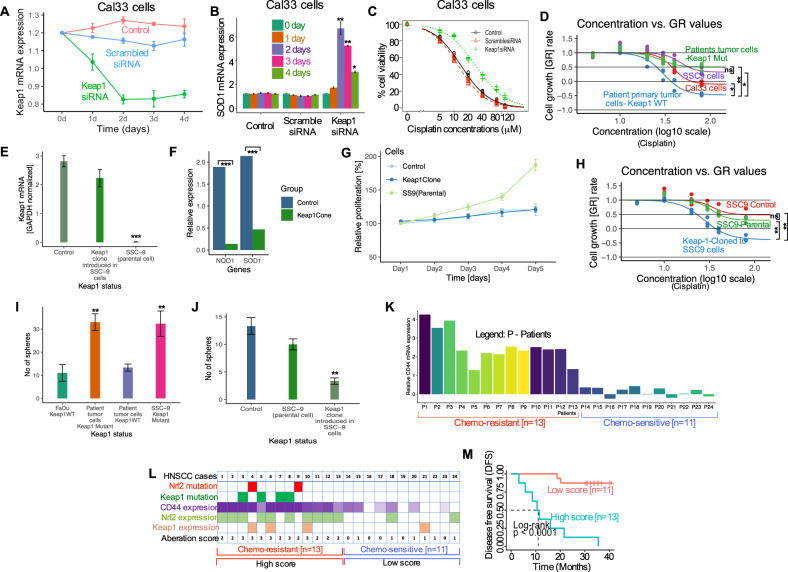
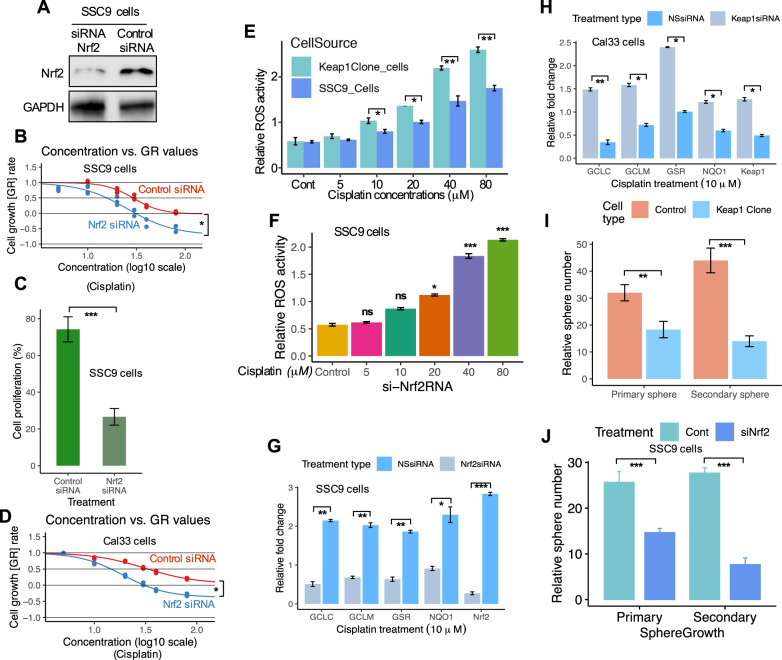
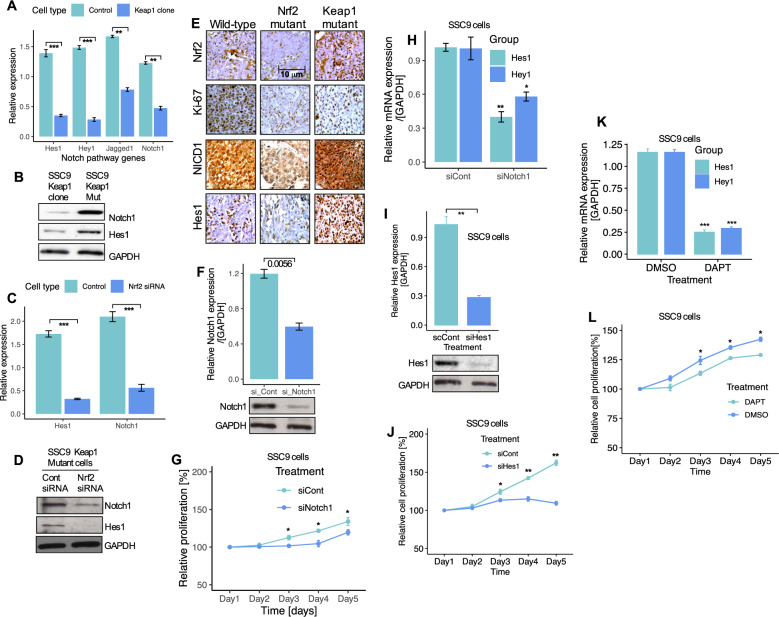
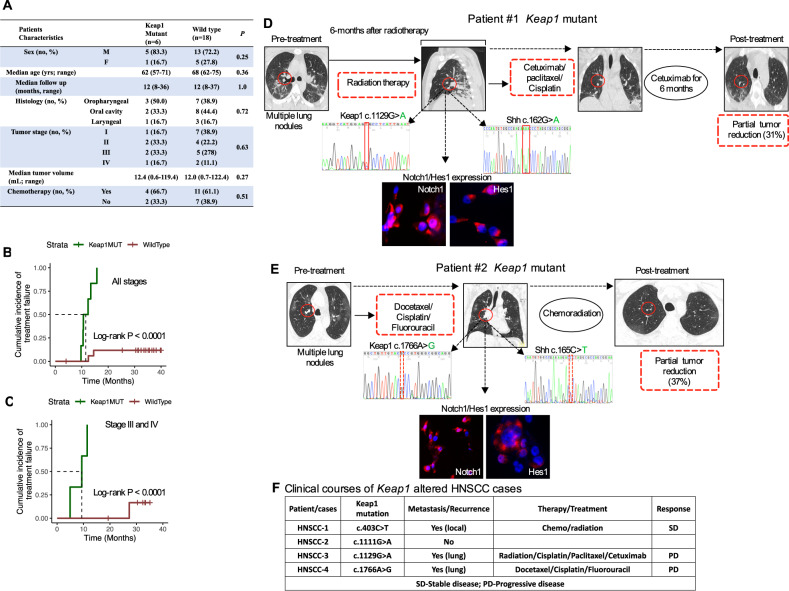
Keap1 mutations regulate Nrf2 activity and lead to chemoresistance in cancers. Yet the underlying molecular mechanisms of chemoresistance are poorly explored. By focusing and genotyping head and neck squamous cell carcinoma (HNSCC) that had available pathologic and clinical data, we provide evidence that Keap1 displays frequent alterations (17%) in HNSCC. Functional loss of Keap1 results in significant activation of Nrf2 and promotes cancer cell growth, proliferation, and elevated cancer stem cell (CSCs) self-renewal efficiency and resistance to oxidative stress. Furthermore, decreased Keap1 activity in these cells increased nuclear accumulation of Nrf2 and activation of the Notch pathway, causing enhanced transcriptional alterations of antioxidants, xenobiotic metabolism enzymes, and resistance to chemotherapeutic treatment. Limiting the Nrf2 activity by either Keap1 complementation or by Nrf2 silencing increased the sensitivity to chemotherapy in Keap1-mutated cells and repressed the CSC self-renewal activity. Our findings suggest that Keap1 mutations define a distinct disease phenotype and the Keap1-Nrf2 pathway is one of the leading molecular mechanisms for clinical chemotherapeutic resistance. Targeting this pathway may provide a potential and attractive personalized treatment strategy for overcoming chemotherapeutic resistance conferred by Keap1 mutations.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
TNFAIP2 confers cisplatin resistance in head and neck squamous cell carcinoma via KEAP1/NRF2 signaling.J Exp Clin Cancer Res. 2023 Aug 1;42(1):190. doi: 10.1186/s13046-023-02775-1. J Exp Clin Cancer Res. 2023. PMID: 37525222 Free PMC article.
-
Gene-expression signature regulated by the KEAP1-NRF2-CUL3 axis is associated with a poor prognosis in head and neck squamous cell cancer.BMC Cancer. 2018 Jan 6;18(1):46. doi: 10.1186/s12885-017-3907-z. BMC Cancer. 2018. PMID: 29306329 Free PMC article.
-
Dysregulation and Epigenetic Reprogramming of NRF2 Signaling Axis Promote Acquisition of Cisplatin Resistance and Metastasis in Head and Neck Squamous Cell Carcinoma.Clin Cancer Res. 2023 Apr 3;29(7):1344-1359. doi: 10.1158/1078-0432.CCR-22-2747. Clin Cancer Res. 2023. PMID: 36689560 Free PMC article.
-
Contradictory roles of Nrf2/Keap1 signaling pathway in cancer prevention/promotion and chemoresistance.DNA Repair (Amst). 2017 Jun;54:13-21. doi: 10.1016/j.dnarep.2017.03.008. Epub 2017 Apr 3. DNA Repair (Amst). 2017. PMID: 28415030 Review.
-
KEAP1/NRF2 (NFE2L2) mutations in NSCLC - Fuel for a superresistant phenotype?Lung Cancer. 2021 Sep;159:10-17. doi: 10.1016/j.lungcan.2021.07.006. Epub 2021 Jul 17. Lung Cancer. 2021. PMID: 34303275 Review.
Cited by
-
KEAP1/NRF2 Mutations in Stem Cells Define an Aggressive Subset of Head and Neck Cancer Patients Who Have a Poor Prognosis, Lung Metastasis, and Therapeutic Failure.Cancers (Basel). 2023 Oct 16;15(20):5006. doi: 10.3390/cancers15205006. Cancers (Basel). 2023. PMID: 37894373 Free PMC article.
-
Multi-omics comprehensive analyses of programmed cell death patterns to regulate the immune characteristics of head and neck squamous cell carcinoma.Transl Oncol. 2024 Mar;41:101862. doi: 10.1016/j.tranon.2023.101862. Epub 2024 Jan 18. Transl Oncol. 2024. PMID: 38237211 Free PMC article.
-
Health Benefits of Coffee Consumption for Cancer and Other Diseases and Mechanisms of Action.Int J Mol Sci. 2023 Jan 31;24(3):2706. doi: 10.3390/ijms24032706. Int J Mol Sci. 2023. PMID: 36769029 Free PMC article. Review.
-
Emerging Role of NRF2 Signaling in Cancer Stem Cell Phenotype.Mol Cells. 2023 Mar 31;46(3):153-164. doi: 10.14348/molcells.2023.2196. Epub 2023 Mar 27. Mol Cells. 2023. PMID: 36994474 Free PMC article. Review.
-
Microfibrillar-associated protein-2 facilitates aggressive progression of oral squamous cell carcinoma cells through Kelch-like E3 ubiquitin ligase-associated protein 1/nuclear factor erythroid 2-related factor 2 signaling pathway.Cytojournal. 2025 Jun 14;22:61. doi: 10.25259/Cytojournal_53_2025. eCollection 2025. Cytojournal. 2025. PMID: 40708830 Free PMC article.
References
-
- López-Verdín S, Lavalle-Carrasco J, Carreón-Burciaga RG, Serafín-Higuera N, Molina-Frechero N, González-González R, et al. Molecular markers of anticancer drug resistance in head and neck squamous cell carcinoma: a literature review. Cancers. 2018;10:376. doi: 10.3390/cancers10100376. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
