

How can assessing hemodynamics help to assess volume status?
- PMID: 35945344
- PMCID: PMC9363272
- DOI: 10.1007/s00134-022-06808-9
How can assessing hemodynamics help to assess volume status?
Abstract
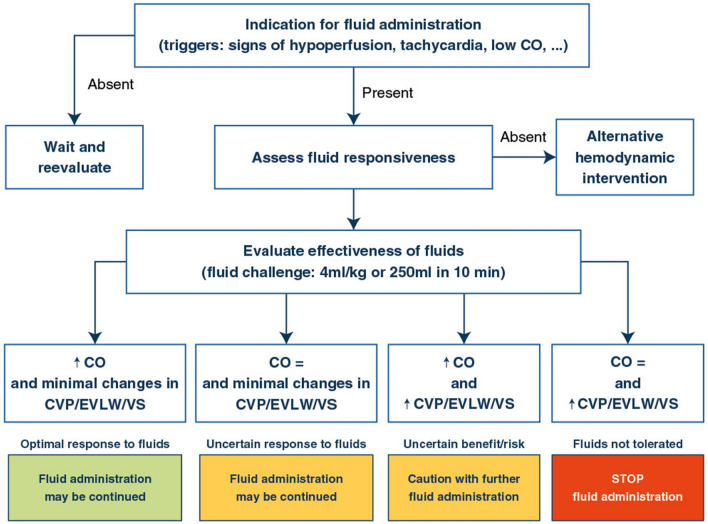
In critically ill patients, fluid infusion is aimed at increasing cardiac output and tissue perfusion. However, it may contribute to fluid overload which may be harmful. Thus, volume status, risks and potential efficacy of fluid administration and/or removal should be carefully evaluated, and monitoring techniques help for this purpose. Central venous pressure is a marker of right ventricular preload. Very low values indicate hypovolemia, while extremely high values suggest fluid harmfulness. The pulmonary artery catheter enables a comprehensive assessment of the hemodynamic profile and is particularly useful for indicating the risk of pulmonary oedema through the pulmonary artery occlusion pressure. Besides cardiac output and preload, transpulmonary thermodilution measures extravascular lung water, which reflects the extent of lung flooding and assesses the risk of fluid infusion. Echocardiography estimates the volume status through intravascular volumes and pressures. Finally, lung ultrasound estimates lung edema. Guided by these variables, the decision to infuse fluid should first consider specific triggers, such as signs of tissue hypoperfusion. Second, benefits and risks of fluid infusion should be weighted. Thereafter, fluid responsiveness should be assessed. Monitoring techniques help for this purpose, especially by providing real time and precise measurements of cardiac output. When decided, fluid resuscitation should be performed through fluid challenges, the effects of which should be assessed through critical endpoints including cardiac output. This comprehensive evaluation of the risk, benefits and efficacy of fluid infusion helps to individualize fluid management, which should be preferred over a fixed restrictive or liberal strategy.
Keywords: Cardiac output; Extravascular lung water; Hypervolemia; Hypovolemia; Tissue edema; Tissue perfusion.
© 2022. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
DDB: Edwards Lifesciences, Philips, Baxter Nadia Aissaoui No conflict of interest. MC: Edwards Lifesciences, Directed Systems. MSC: Edwards Lifesciences. AD: Edwards Lifesciences, Masimo. LH: No conflict of interest. GH: No conflict of interest. AM: Vygon, Edwards, Philips and Getinge. SM: No conflict of interest. MO: Fresenius Medical, Baxter, Biomerieux. MRP: Edwards LifeSciences, Baxter, Intelomed, Exostat. J-LT: Getinge. PV: Baxter. J-LV: No conflict of interest. XM: Gettinge.
Figures
Comment in
-
Echocardiography and volume status: lessons from left ventricular assist devices.Intensive Care Med. 2022 Dec;48(12):1820-1821. doi: 10.1007/s00134-022-06870-3. Epub 2022 Oct 5. Intensive Care Med. 2022. PMID: 36197497 No abstract available.
Dataset use reported in
-
Chronic cardiac disease should be considered when using left ventricular dimensions to assess volume status and fluid responsiveness.Intensive Care Med. 2022 Dec;48(12):1822-1824. doi: 10.1007/s00134-022-06895-8. Epub 2022 Oct 5. Intensive Care Med. 2022. PMID: 36197495 No abstract available.
References
-
- Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, Machado FR, McIntyre L, Ostermann M, Prescott HC, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47:1181–1247. doi: 10.1007/s00134-021-06506-y. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
