

Efficacy and safety of the investigational complement C5 inhibitor zilucoplan in patients hospitalized with COVID-19: an open-label randomized controlled trial
- PMID: 35945604
- PMCID: PMC9361275
- DOI: 10.1186/s12931-022-02126-2
Efficacy and safety of the investigational complement C5 inhibitor zilucoplan in patients hospitalized with COVID-19: an open-label randomized controlled trial
Abstract
Background: The efficacy and safety of complement inhibition in COVID-19 patients is unclear.
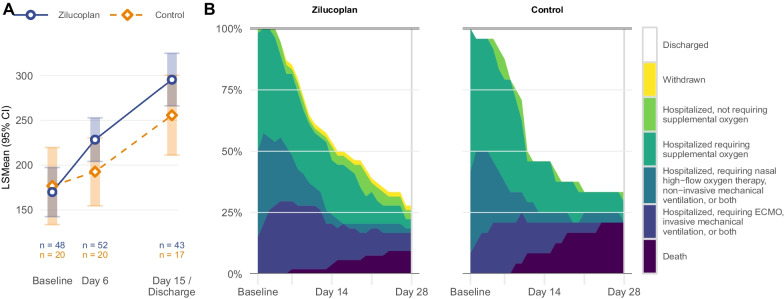
Methods: A multicenter randomized controlled, open-label trial. Hospitalized COVID-19 patients with signs of systemic inflammation and hypoxemia (PaO2/FiO2 below 350 mmHg) were randomized (2:1 ratio) to receive standard of care with or without the C5 inhibitor zilucoplan daily for 14 days, under antibiotic prophylaxis. The primary outcome was improvement in oxygenation at day 6 and 15.
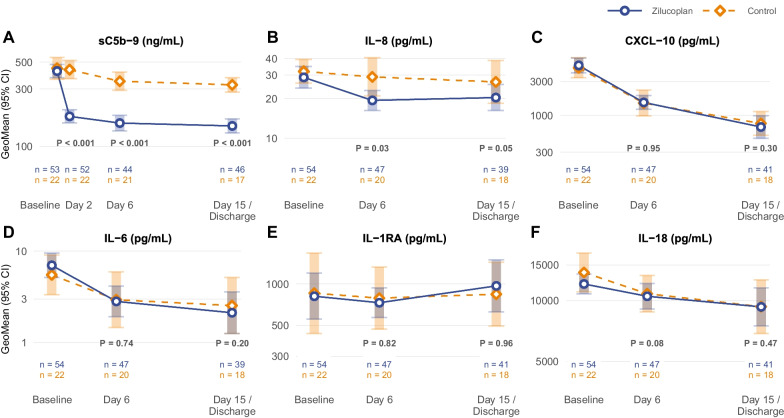
Results: 81 patients were randomly assigned to zilucoplan (n = 55) or the control group (n = 26). 78 patients were included in the safety and primary analysis. Most were men (87%) and the median age was 63 years. The mean improvement in PaO2/FiO2 from baseline to day 6 was 56.4 mmHg in the zilucoplan group and 20.6 mmHg in the control group (mean difference + 35.8; 95% confidence interval (CI) - 9.4 to 80.9; p = 0.12), an effect also observed at day 15. Day 28 mortality was 9% in the zilucoplan and 21% in the control group (odds ratio 0.4; 95% CI 0.1 to 1.5). At long-term follow up, the distance walked in a 6-min test was 539.7 m in zilucoplan and 490.6 m in the control group (p = 0.18). Zilucoplan lowered serum C5b-9 (p < 0.001) and interleukin-8 (p = 0.03) concentration compared with control. No relevant safety differences between the zilucoplan and control group were identified.
Conclusion: Administration of zilucoplan to COVID-19 patients in this proof-of-concept randomized trial was well tolerated under antibiotic prophylaxis. While not reaching statistical significance, indicators of respiratory function (PaO2/FiO2) and clinical outcome (mortality and 6-min walk test) suggest that C5 inhibition might be beneficial, although this requires further research in larger randomized studies.
Trial registration: ClinicalTrials.gov NCT04382755.
Keywords: COVID-19; Complement 5; Complement system; Systemic inflammation.
© 2022. The Author(s).
Conflict of interest statement
CeB, EDL, JoD, BM, KVD have received an FWO PhD Fellowship. ND, JuD, SJT have received an FWO Postdoctoral Grant. ClB, LD, SG, ML, TS are employed by UCB. VP is employed by Sillar Clinical N.V. ClB, LD, ML, TS hold stock or stock options from UCB. LD holds stock or stock options from Sanofi. TS holds stock or stock options from Pfizer and Lilly. ClB, BNL, EVB have contributed or participated on a DSMB or Advisory Board. BNL has received a grant from Partner Therapeutics, Inc., has received consulting fees and payments from Sanofi and GSK and holds stock options from Argenx. EVB has received a grant from Ghent University, is principal investigator in a trial sponsored by Exevir Bio and has received consulting fees or payments from GSK, MDS and Gilead. ID, NDN, PD, EG, FH, TH, CK, SL, MM, WT, SV report no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
