

Effect of goal-directed haemodynamic therapy guided by non-invasive monitoring on perioperative complications in elderly hip fracture patients within an enhanced recovery pathway
- PMID: 35945605
- PMCID: PMC9364538
- DOI: 10.1186/s13741-022-00277-w
Effect of goal-directed haemodynamic therapy guided by non-invasive monitoring on perioperative complications in elderly hip fracture patients within an enhanced recovery pathway
Abstract
Background: Goal-directed haemodynamic therapy (GDHT) has been shown to reduce morbidity and mortality in high-risk surgical patients. However, there is little evidence of its efficacy in patients undergoing hip fracture surgery. This study aims to evaluate the effect of GDHT guided by non-invasive haemodynamic monitoring on perioperative complications in patients undergoing hip fracture surgery.
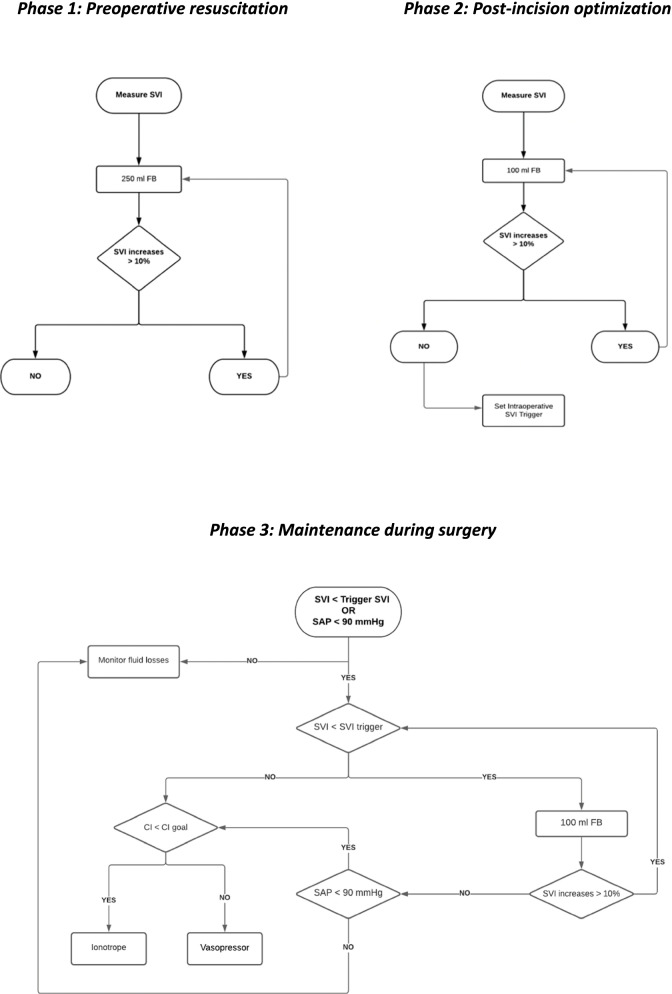
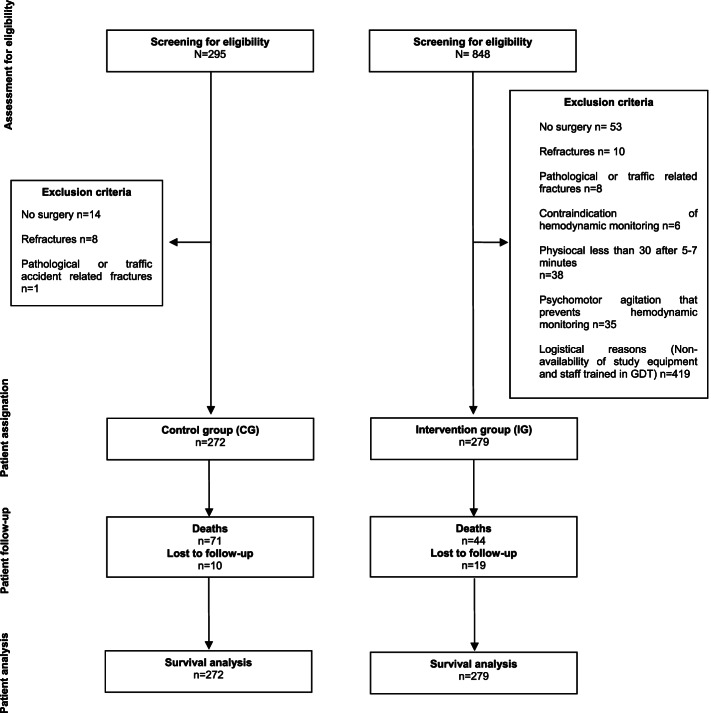
Methods: Patients > 64 years undergoing hip fracture surgery within an enhanced recovery pathway (ERP) were enrolled in this single-centre, non-randomized, intervention study with a historical control group and 12-month follow-up. Exclusion criteria were patients with pathological fractures, traffic-related fractures and refractures. Control group (CG) patients received standard care treatment. Intervention group (IG) patients received a GDHT protocol based on achieving an optimal stroke volume, in addition to a systolic blood pressure > 90 mmHg and an individualized cardiac index. No changes were made between groups in the ERP during the study period. Primary outcome was percentage of patients who developed intraoperative haemodynamic instability. Secondary outcomes were intraoperative arrhythmias, postoperative complications (cardiovascular, respiratory, infectious and renal complications), administered fluids, vasopressor requirements, perioperative transfusion, length of hospital stay, readmission and 1-year survival.
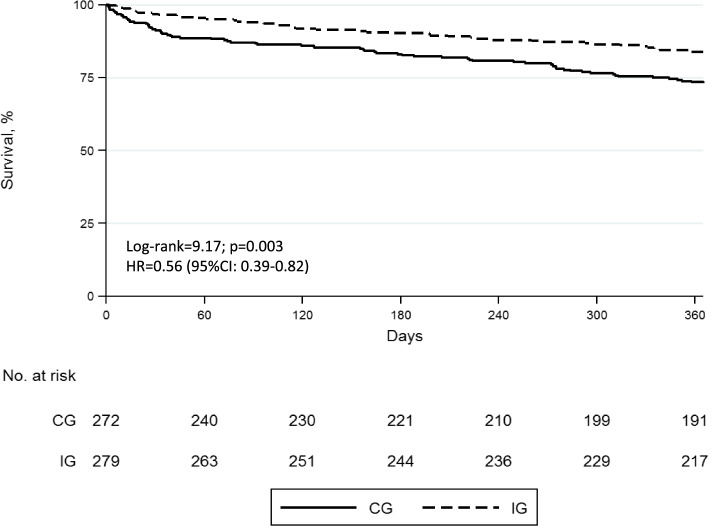
Results: In total, 551 patients (CG=272; IG=279) were included. Intraoperative haemodynamic instability was lower in the IG (37.5% vs 28.0%; p=0.017). GDHT patients had fewer postoperative cardiovascular (18.8% vs 7.2%; p < 0.001), respiratory (15.1% vs 3.6%; p<0.001) and infectious complications (21% vs 3.9%; p<0.001) but not renal (12.1% vs 33.7%; p<0.001). IG patients had less vasopressor requirements (25.5% vs 39.7%; p<0.001) and received less fluids [2.600 ml (IQR 1700 to 2700) vs 850 ml (IQR 750 to 1050); p=0.001] than control group. Fewer patients required transfusion in GDHT group (73.5% vs 44.4%; p<0.001). For IG patients, median length of hospital stay was shorter [11 days (IQR 8 to 16) vs 8 days; (IQR 6 to 11) p < 0.001] and 1-year survival higher [73.4% (95%CI 67.7 to 78.3 vs 83.8% (95%CI 78.8 to 87.7) p<0.003].
Conclusions: The use of GDHT decreases intraoperative complications and postoperative cardiovascular, respiratory and infectious but not postoperative renal complications. This strategy was associated with a shorter hospital stay and increased 1-year survival.
Trial registration: ClinicalTrials.gov NCT02479321 .
Keywords: Enhanced recovery after surgery; Enhanced recovery pathway; Fluid therapy; Goal-directed haemodynamic therapy; Hip fracture; Intraoperative complications; Mortality; postoperative complications.
© 2022. The Author(s).
Conflict of interest statement
Dr Lorente, Dr Jiménez, Dr Ripollés-Melchor and Dr Monge have received conference fees from Edwards Lifesciences.
Dr Lorente & Dr Ripollés-Melchor have received conference fees from Fresenius Kabi and bioMérieux.
Dr Ripollés-Melchor & Dr Monge have received conference fees from Dextera Medical.
Dr Lorente has received conference fees from Vifor Pharma, Grifols and financial support for research obtained through Edwards Lifesciences Grant Portal. Economic research support from bioMérieux.
Dr Ripollés-Melchor has received conference fees from MSD.
The rest of the authors declare that they have competing interests.
Figures
Similar articles
-
Towards individualized perioperative, goal-directed haemodynamic algorithms for patients of advanced age: observations during a randomized controlled trial (NCT01141894).Br J Anaesth. 2016 Apr;116(4):486-92. doi: 10.1093/bja/aew025. Br J Anaesth. 2016. PMID: 26994228 Clinical Trial.
-
Effect of goal-directed haemodynamic therapy on postoperative complications in low-moderate risk surgical patients: a multicentre randomised controlled trial (FEDORA trial).Br J Anaesth. 2018 Apr;120(4):734-744. doi: 10.1016/j.bja.2017.12.018. Epub 2018 Feb 3. Br J Anaesth. 2018. PMID: 29576114 Clinical Trial.
-
Effect of postoperative goal-directed therapy in cancer patients undergoing high-risk surgery: a randomized clinical trial and meta-analysis.Crit Care. 2018 May 23;22(1):133. doi: 10.1186/s13054-018-2055-4. Crit Care. 2018. PMID: 29792232 Free PMC article. Clinical Trial.
-
LiDCO-based fluid management in patients undergoing hip fracture surgery under spinal anaesthesia: a randomized trial and systematic review.Br J Anaesth. 2015 Mar;114(3):444-59. doi: 10.1093/bja/aeu386. Epub 2014 Dec 11. Br J Anaesth. 2015. PMID: 25500940 Clinical Trial.
-
Goal-directed haemodynamic therapy during general anaesthesia for noncardiac surgery: a systematic review and meta-analysis.Br J Anaesth. 2022 Mar;128(3):416-433. doi: 10.1016/j.bja.2021.10.046. Epub 2021 Dec 13. Br J Anaesth. 2022. PMID: 34916049 Free PMC article.
Cited by
-
Liberal intraoperative fluid management leads to increased complication rates in geriatric patients with hip fracture.Eur J Trauma Emerg Surg. 2023 Dec;49(6):2485-2493. doi: 10.1007/s00068-023-02326-5. Epub 2023 Jul 12. Eur J Trauma Emerg Surg. 2023. PMID: 37436466
-
Preoperative goal directed therapy in geriatric hip fracture patients - a retrospective quality improvement study.BMC Geriatr. 2024 Nov 18;24(1):959. doi: 10.1186/s12877-024-05554-5. BMC Geriatr. 2024. PMID: 39558199 Free PMC article.
