

Clinical sepsis phenotypes in critically ill COVID-19 patients
- PMID: 35945618
- PMCID: PMC9361232
- DOI: 10.1186/s13054-022-04118-6
Clinical sepsis phenotypes in critically ill COVID-19 patients
Abstract
Background: A greater understanding of disease heterogeneity may facilitate precision medicine for coronavirus disease 2019 (COVID-19). Previous work identified four distinct clinical phenotypes associated with outcome and treatment responses in non-COVID-19 sepsis patients, but it is unknown if and how these phenotypes are recapitulated in COVID-19 sepsis patients.
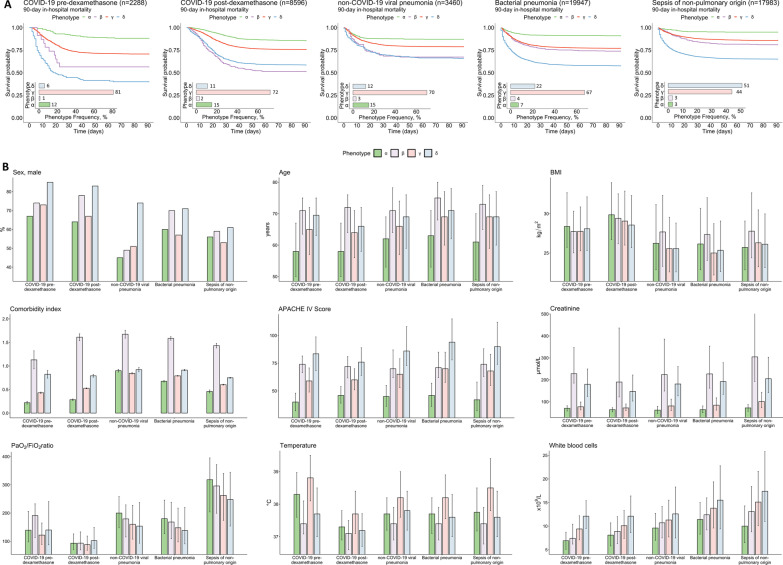
Methods: We applied the four non-COVID-19 sepsis phenotypes to a total of 52,274 critically ill patients, comprising two cohorts of COVID-19 sepsis patients (admitted before and after the introduction of dexamethasone as standard treatment) and three non-COVID-19 sepsis cohorts (non-COVID-19 viral pneumonia sepsis, bacterial pneumonia sepsis, and bacterial sepsis of non-pulmonary origin). Differences in proportions of phenotypes and their associated mortality were determined across these cohorts.
Results: Phenotype distribution was highly similar between COVID-19 and non-COVID-19 viral pneumonia sepsis cohorts, whereas the proportion of patients with the δ-phenotype was greater in both bacterial sepsis cohorts compared to the viral sepsis cohorts. The introduction of dexamethasone treatment was associated with an increased proportion of patients with the δ-phenotype (6% vs. 11% in the pre- and post-dexamethasone COVID-19 cohorts, respectively, p < 0.001). Across the cohorts, the α-phenotype was associated with the most favorable outcome, while the δ-phenotype was associated with the highest mortality. Survival of the δ-phenotype was markedly higher following the introduction of dexamethasone (60% vs 41%, p < 0.001), whereas no relevant differences in survival were observed for the other phenotypes among COVID-19 patients.
Conclusions: Classification of critically ill COVID-19 patients into clinical phenotypes may aid prognostication, prediction of treatment efficacy, and facilitation of personalized medicine.
Keywords: COVID-19; Dexamethasone; Personalized medicine; Phenotypes; Sepsis.
© 2022. The Author(s).
Conflict of interest statement
Not applicable.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
