

Blocking RAGE improves wound healing in diabetic pigs
- PMID: 35945908
- PMCID: PMC9927915
- DOI: 10.1111/iwj.13909
Blocking RAGE improves wound healing in diabetic pigs
Abstract
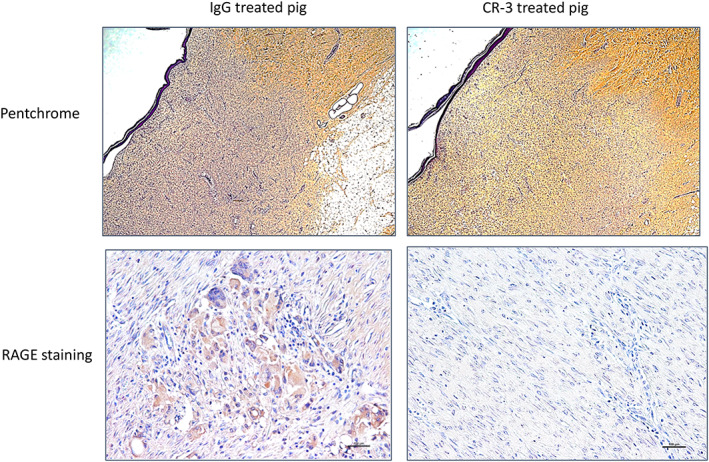
Receptor for Advanced Glycated End-products (RAGE) is highly expressed in diabetes and impairs wound healing. We proposed that administering an antibody that blocks RAGE will hasten the healing of dorsal wounds in diabetic pigs compared with a non-immune IgG. Two purpose-bred diabetic (D) Yucatan minipigs (Sinclair, Auxvasse MO) each underwent 12 2 × 2 cm full thickness dorsal wounds: four wounds received decellularized porcine skin patches (Xylyx Bio, Bklyn NY): four anti-RAGE Ab (CR-3) infused patches, four saline infused patches and four wounds were left open. One pig received anti-RAGE Ab (CR-3) 1 mg/kg IM q 10 days and other received non-immune IgG. Wounds were measured at 2 and 4 weeks followed by euthanasia and wound harvesting. At 2 weeks few of the patches appeared to be incorporated into the wound. By 4 weeks all patches in pigs treated systemically with CR-3 were detached and the wounds almost healed. For all 24 wounds for both pigs regardless of presence of patch or type of patch, the average IgG treated pig wound size at 4 weeks was 69.2 ± 14.6% of initial size and the average CR-3 treated pig wound size was 40.9 ± 11.3% of initial size (P = 0.0002). Quantitative immunohistology showed greater staining for collagen in the CR-3 treated wounds compared with IgG treated. Staining was positive for RAGE, Mac, and IL-6 in the IgG treated wounds and negative in the CR-3 treated wounds. From these pilot experiments, we conclude that a RAGE blocking antibody given parenterally improved wound healing in a diabetic pig while patches were not effective.
Keywords: RAGE; diabetes; wound healing.
© 2022 The Authors. International Wound Journal published by Medicalhelplines.com Inc and John Wiley & Sons Ltd.
Figures





References
-
- Fowkes FG, Aboyans V, Fowkes FJI, McDermott MM, Sampson UKA, Criqui MH. Peripheral artery disease: epidemiology and global perspectives. Nat Rev Cardiol. 2017;14(3):156‐170. - PubMed
-
- Eldrup N, Sillesen H, Prescott E, Nordestgaard BG. Ankle brachial index, C‐reactive protein, and central augmentation index to identify individuals with severe atherosclerosis. Eur Heart J. 2006;27(3):316‐322. - PubMed
-
- Anand SS, Caron F, Eikelboom JW, et al. Major adverse limb events and mortality in patients with peripheral artery disease: the COMPASS trial. J Am Coll Cardiol. 2018;71(20):2306‐2315. - PubMed
-
- Low Wang CC, Blomster JI, Heizer G, et al. Cardiovascular and limb outcomes in patients with diabetes and peripheral artery disease: the EUCLID trial. J Am Coll Cardiol. 2018;72(25):3274‐3284. - PubMed
-
- Boulton AJ, Vileikyte L, Ragnarson‐Tennvall G, Apelqvist J. The global burden of diabetic foot disease. Lancet. 2005;366(9498):1719‐1724. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
