Spectrum of Surgically Resected Lesions of the Cavernous Sinus: A Neuropathologic Audit
- PMID: 35946008
- PMCID: PMC9357489
- DOI: 10.1055/s-0042-1750707
Spectrum of Surgically Resected Lesions of the Cavernous Sinus: A Neuropathologic Audit
Abstract
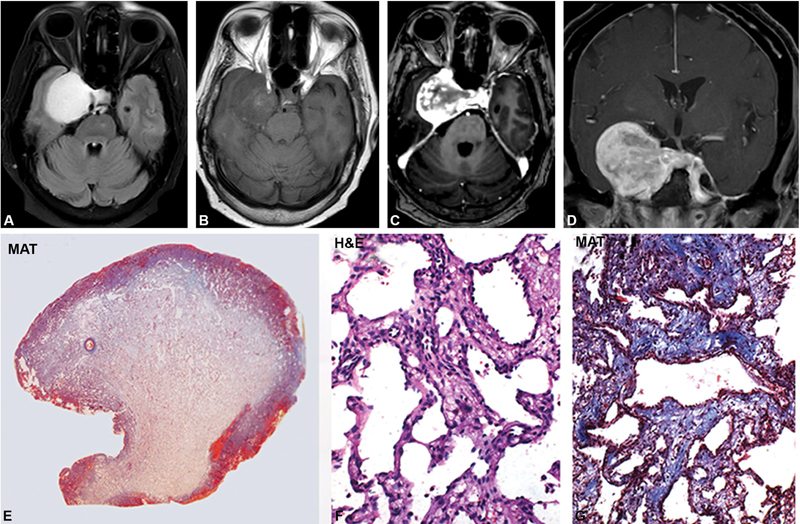
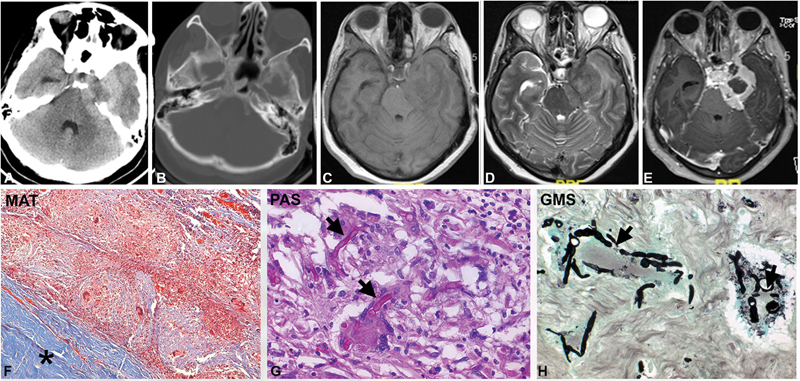
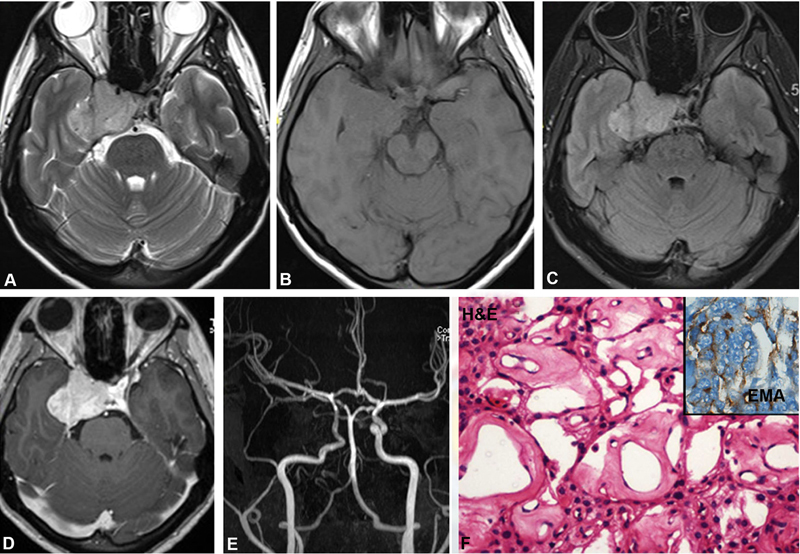
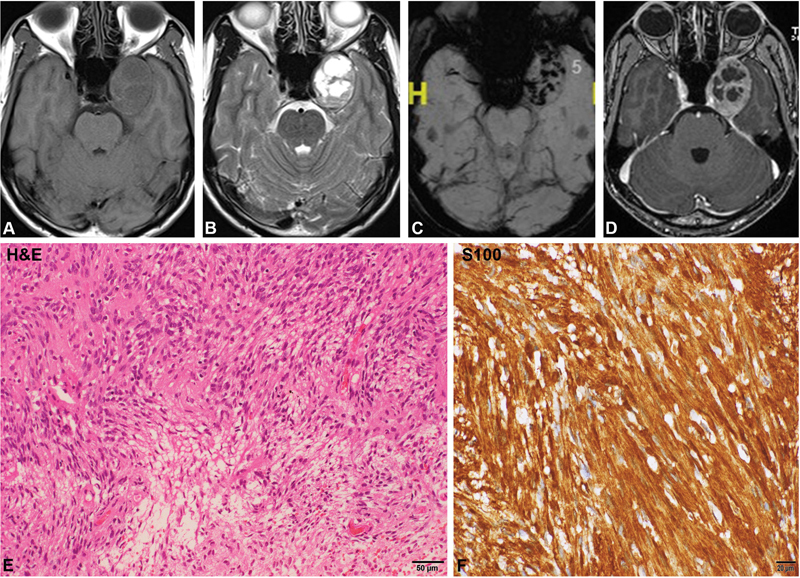
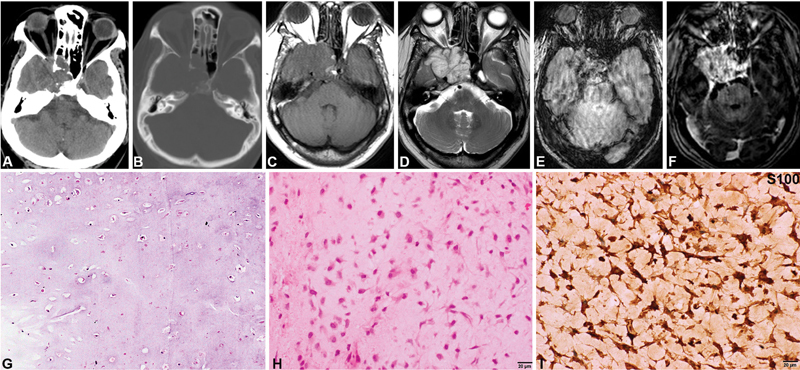
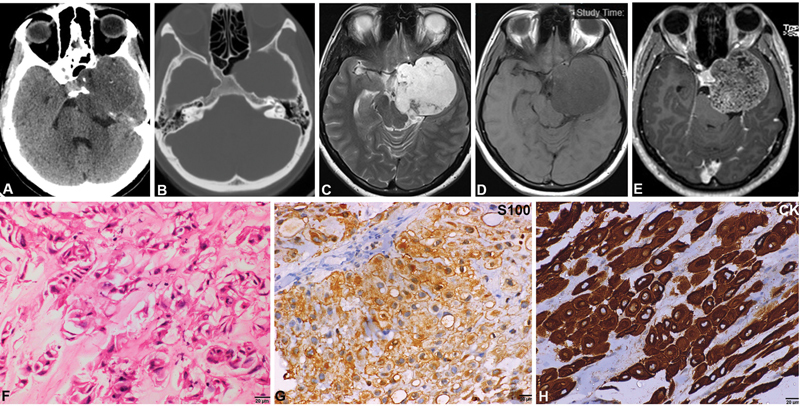
Background The cavernous sinus is a complex space composed of extradural venous plexus within dural folds. Several important structures like the carotid artery, cranial nerves, and sympathetic nerve fibers traverse through this space. Radiological diagnosis may not be definitive and in the context of discordance between clinical and neuroimaging diagnosis, histopathological evaluation becomes essential for diagnosis and management. Literature on the pathological spectrum of lesions is scarce as, with a shift in the treatment paradigm, most small lesions of cavernous sinus are treated with radiosurgery. However, surgical management still plays a role for larger lesions and in radiologically ambiguous cases for planning the definitive management. Materials and Methods We retrospectively reviewed all surgically resected lesions of the cavernous sinus over the last two decades (1998-2019). The clinical presentation, neuroimaging features, and histopathological findings were reviewed. Lesions extending from sella and other adjacent areas were excluded. Results Thirty-eight cases of isolated cavernous sinus mass lesions were diagnosed over the last two decades (1998-2019). Cavernous hemangiomas (19 cases, 50%) constituted the most frequent pathology, followed by aspergilloma, meningioma, schwannoma, metastatic adenocarcinoma, chondrosarcoma, and chordoma. Overall, 29.4% (10/34) could not be accurately diagnosed on neuroimaging. Of these, four cases of cavernous hemangiomas were mistaken for either meningioma (three cases) or schwannoma (one case). Neither chordoma nor chondrosarcoma was suspected. Conclusion This is the first study in literature, enumerating the pathological and imaging spectrum of surgically resected cavernous sinus lesions. Cavernous hemangiomas, metastases and chordomas, and chondrosarcoma posed the greatest difficulty in diagnosis on neuroimaging and the reasons for the same are analyzed. In the context of clinical and neuroimaging discordance in diagnosis, pathological characterization becomes essential for appropriate and timely management.
Keywords: cavernous sinus; histopathology; imaging.
Association for Helping Neurosurgical Sick People. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of interest None declared.
Figures

References
-
- Larson T L. Petrous apex and cavernous sinus: anatomy and pathology. Semin Ultrasound CT MR. 1993;14(03):232–246. - PubMed
-
- Keane J R. Cavernous sinus syndrome. Analysis of 151 cases. Arch Neurol. 1996;53(10):967–971. - PubMed
-
- Nakamura M, Krauss J K. Image-guided resection of small lesions in the cavernous sinus and Meckel's cave. Eur J Surg Oncol. 2010;36(02):208–213. - PubMed
-
- Fratzoglou M, Condilis N, Panayiotopoulos V, Bahal D, Patheni M. Cavernous sinus chondroma. Case report and review of the literature. Ann Ital Chir. 2008;79(01):43–45. - PubMed