

Can cannabis kill? Characteristics of deaths following cannabis use in England (1998-2020)
- PMID: 35946604
- PMCID: PMC9716494
- DOI: 10.1177/02698811221115760
Can cannabis kill? Characteristics of deaths following cannabis use in England (1998-2020)
Abstract
Background: Cannabis is the most widely used illegal drug but is rarely considered a causal factor in death.
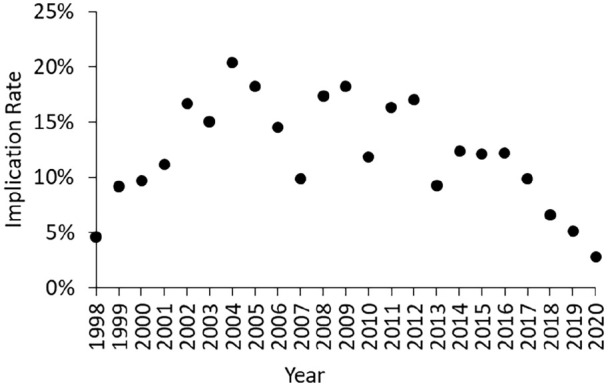
Aims: This study aimed to understand trends in deaths in England where cannabinoids were detected at post-mortem, and to evaluate the clinical utility of post-mortem cannabinoid concentrations in coronial investigations.
Methods: Deaths with cannabinoid detections reported to the National Programme on Substance Abuse Deaths (NPSAD) were extracted and analysed.
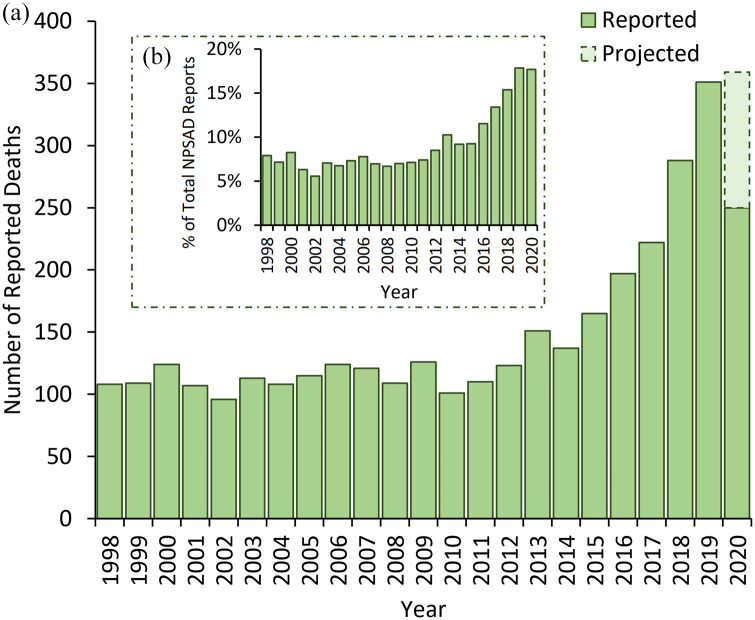
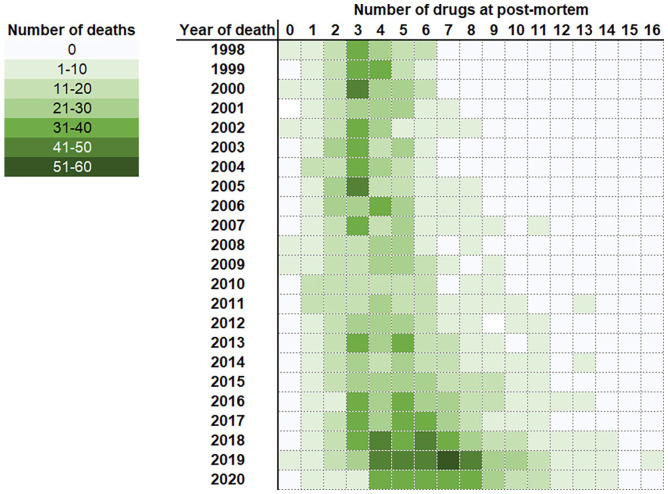
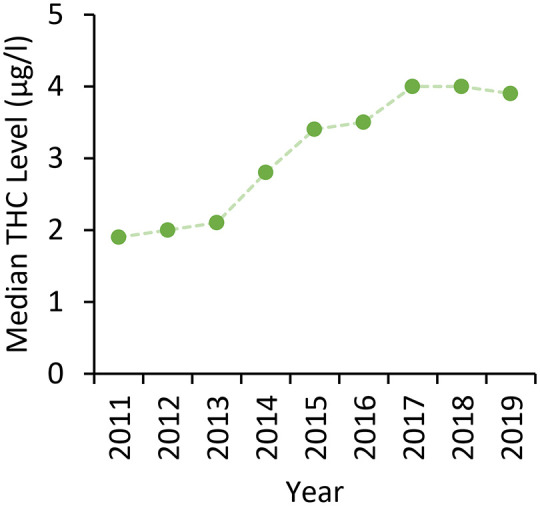
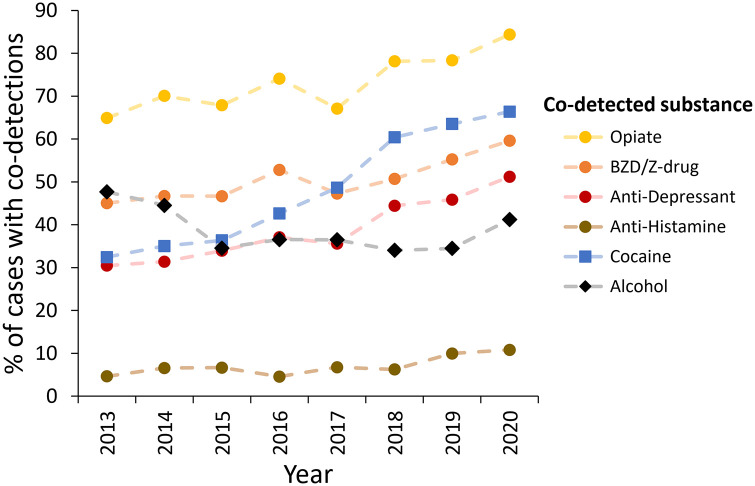
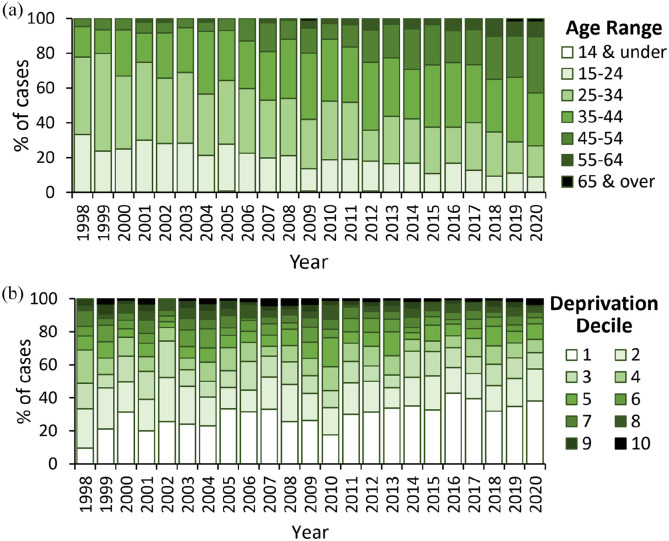
Results: From 1998 to 2011, on average 7% of all cases reported to NPSAD had a cannabinoid detected (n = 110 deaths per year), rising to 18% in 2020 (n = 350). Death following cannabis use alone was rare (4% of cases, n = 136/3455). Traumatic injury was the prevalent underlying cause in these cases (62%, n = 84/136), with cannabis toxicity cited in a single case. Polydrug use was evident in most cases (96%, n = 3319/3455), with acute drug toxicity the prevalent underlying cause (74%, n = 2458/3319). Cardiac complications were the most cited physiological underlying cause of death (4%, n = 144/3455). The median average Δ9-tetrahydrocannabinol post-mortem blood concentrations were several magnitudes lower than previously reported median blood concentrations in living users (cannabis alone: 4.3 µg/L; cannabis in combination with other drugs: 3.5 µg/L).
Conclusions: Risk of death due to cannabis toxicity is negligible. However, cannabis can prove fatal in circumstances with risk of traumatic physical injury, or in individuals with cardiac pathophysiologies. These indirect harms need careful consideration and further study to better elucidate the role cannabis plays in drug-related mortality. Furthermore, the relevance of cannabinoid quantifications in determining cause of death in coronial investigations is limited.
Keywords: Cannabis; THC; cannabinoids; drug-related death; toxicity; Δ9-tetrahydrocannabinol.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
