

Acetabular orientation in triple pelvic osteotomy: is intraoperative fluoroscopy reliable?
- PMID: 35947170
- PMCID: PMC10293451
- DOI: 10.1007/s00402-022-04568-1
Acetabular orientation in triple pelvic osteotomy: is intraoperative fluoroscopy reliable?
Abstract
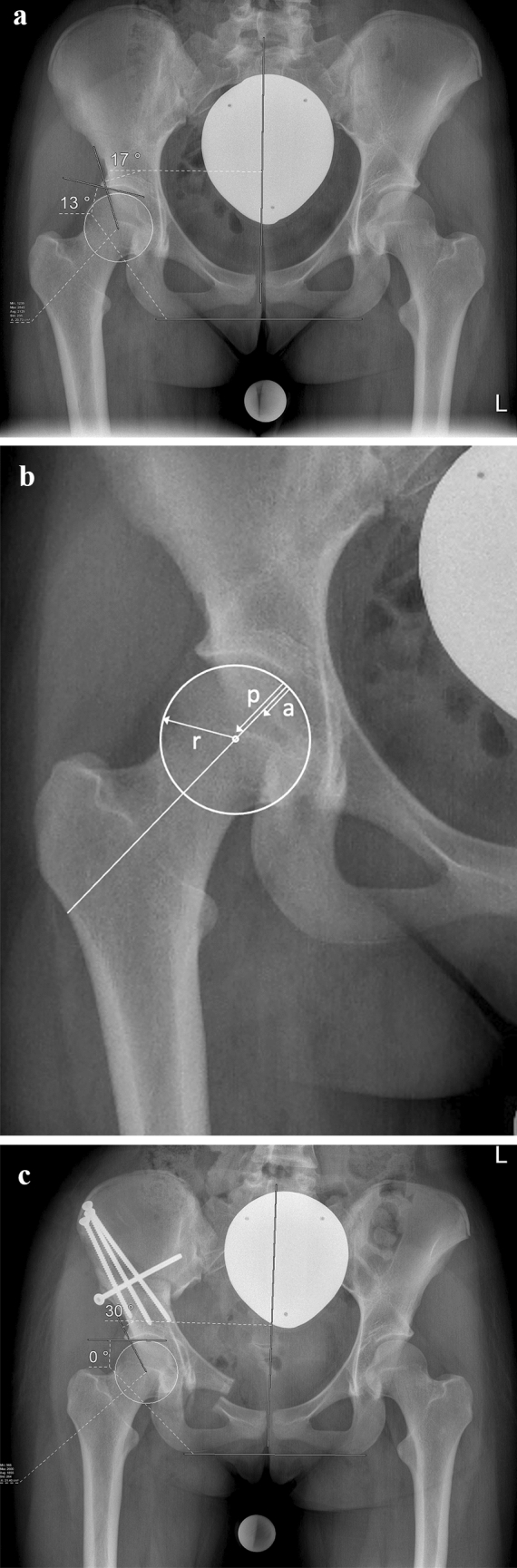
Purpose: In pelvic osteotomies, unfavorable balancing of the anterior and posterior acetabular wall can affect the longevity of the natural joint. This raises the question, whether intraoperative fluoroscopy is sufficiently accurate. The objective was to assess the correlation between acetabular parameters [lateral center edge angle (LCEA), acetabular index (AI), anterior wall index (AWI), posterior wall index (PWI)] acquired on intraoperative fluoroscopic images and postoperative pelvic radiographs and to analyze intra- and interobserver reliability of these parameters.
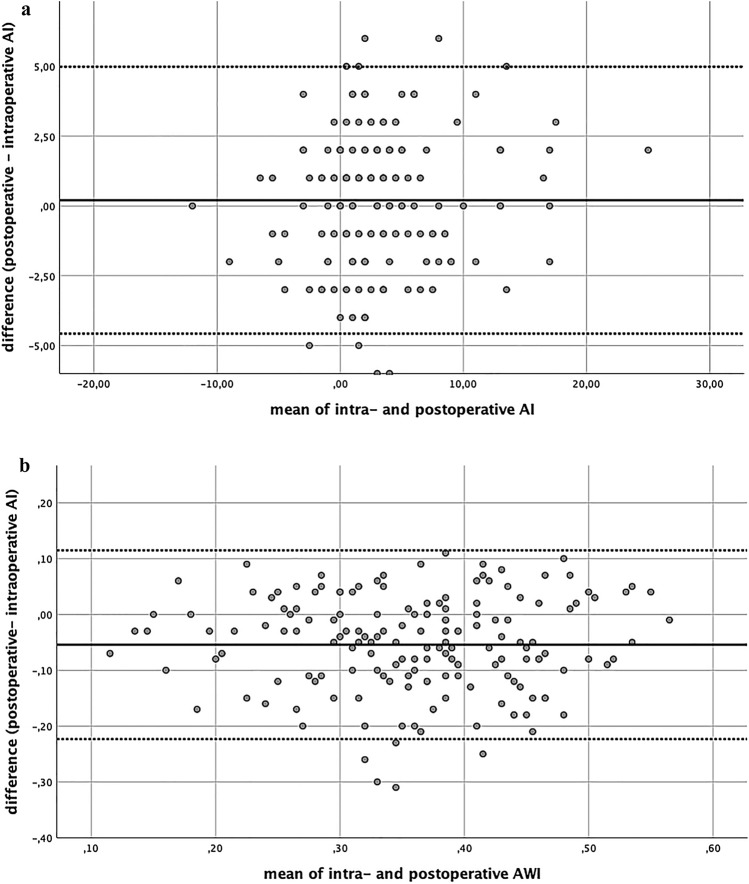
Methods: A retrospective examination was conducted on 206 consecutive cases (176 patients) after triple pelvic osteotomy (TPO). Every patient received a pre- and postoperative pelvic radiograph in supine position in exactly the same technique. A highly standardized surgical sequence allowed consistent intraoperative fluoroscopic imaging. LCAE, AI, PWI and AWI were measured by an experienced orthopedic surgeon and an orthopedic surgeon in training. Statistics comprised a priori power analysis, Bland-Altman analysis and intraclass correlation coefficient (ICC).
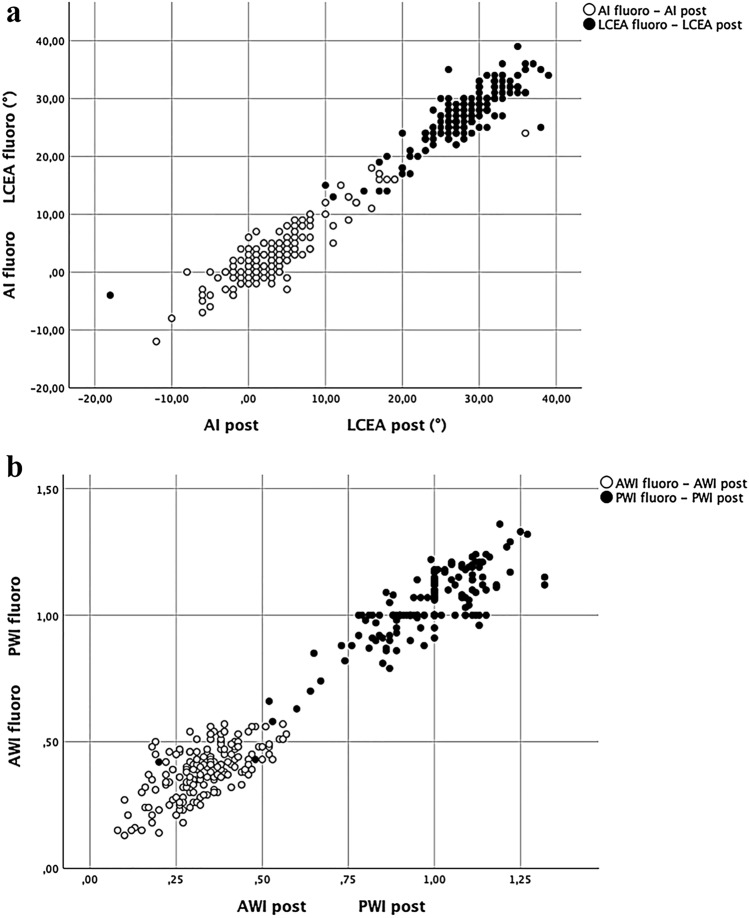
Results: A total of 165 cases were included. ICC between the parameters of the fluoroscopic images and postoperative radiographs was for LCEA: 0.935, AI: 0.936, AWI: 0.725 and PWI: 0.878. Intraobserver ICC for all parameters ranged from 0.953 to 0.989, interobserver ICC from 0.798 to 0.968, respectively.
Conclusion: In the surgical treatment of hip dysplasia by means of TPO, intraoperative fluoroscopic imaging has proven to be reliable and accurate. Intraobserver correlation was excellent for all parameters. The correlation between the intraoperative fluoroscopic images and postoperative radiographs ranged from good to excellent, with the lowest values for the acetabular wall indices (AWI and PWI).
Keywords: Hip dysplasia; Hip joint preservation; Intraoperative fluoroscopy; Surgery; Triple pelvic osteotomy.
© 2022. The Author(s).
Conflict of interest statement
The authors have no financial or non-financial interest to disclose.
Figures
Similar articles
-
What Is the Reliability and Accuracy of Intraoperative Fluoroscopy in Evaluating Anterior, Lateral, and Posterior Coverage During Periacetabular Osteotomy?Clin Orthop Relat Res. 2019 May;477(5):1138-1144. doi: 10.1097/CORR.0000000000000616. Clin Orthop Relat Res. 2019. PMID: 30676406 Free PMC article.
-
What is the agreement between intraoperative fluoroscopy and postoperative radiographs in Bernese periacetabular osteotomy?BMC Musculoskelet Disord. 2022 Dec 30;23(1):1139. doi: 10.1186/s12891-022-06054-6. BMC Musculoskelet Disord. 2022. PMID: 36581915 Free PMC article.
-
Treatment of borderline hip dysplasia with triple pelvic osteotomy: preoperative values of acetabular index and lateral center edge angle can indicate overcorrection.Arch Orthop Trauma Surg. 2023 Oct;143(10):6139-6146. doi: 10.1007/s00402-023-04920-z. Epub 2023 Jun 5. Arch Orthop Trauma Surg. 2023. PMID: 37272987 Free PMC article.
-
Operative Fluoroscopic Correction Is Reliable and Correlates With Postoperative Radiographic Correction in Periacetabular Osteotomy.Clin Orthop Relat Res. 2017 Apr;475(4):1100-1106. doi: 10.1007/s11999-016-5071-1. Clin Orthop Relat Res. 2017. PMID: 27620804 Free PMC article.
-
Dilemmas in imaging for peri-acetabular osteotomy: the influence of patient position and imaging technique on the radiological features of hip dysplasia.Bone Joint J. 2014 Sep;96-B(9):1155-60. doi: 10.1302/0301-620X.96B9.34269. Bone Joint J. 2014. PMID: 25183583 Review.
Cited by
-
Age and magnitude of acetabular correction impair bone healing after triple pelvic osteotomy.Arch Orthop Trauma Surg. 2023 Nov;143(11):6599-6607. doi: 10.1007/s00402-023-04966-z. Epub 2023 Jul 8. Arch Orthop Trauma Surg. 2023. PMID: 37421516 Free PMC article.
-
Effects of different pelvic osteotomies on acetabular morphology in developmental dysplasia of hip in children.World J Orthop. 2023 Apr 18;14(4):186-196. doi: 10.5312/wjo.v14.i4.186. eCollection 2023 Apr 18. World J Orthop. 2023. PMID: 37155509 Free PMC article. Review.
-
Three-dimensional acetabular reorientation during periacetabular osteotomy: an intraoperative navigation method using an external fixator for periacetabular osteotomy.Arch Orthop Trauma Surg. 2024 Nov;144(11):4969-4977. doi: 10.1007/s00402-024-05590-1. Epub 2024 Sep 24. Arch Orthop Trauma Surg. 2024. PMID: 39313642
References
-
- Lerch TD, Steppacher SD, Liechti EF, Tannast M, Siebenrock KA. One-third of hips after periacetabular osteotomy survive 30 years with good clinical results, no progression of arthritis, or conversion to THA. Clin Orthop Relat Res. 2017;475(4):1154–1168. doi: 10.1007/s11999-016-5169-5. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
