

Use of Electrocardiogram Monitoring in Adult Patients Taking High-Risk QT Interval Prolonging Medicines in Clinical Practice: Systematic Review and Meta-analysis
- PMID: 35947343
- PMCID: PMC9492585
- DOI: 10.1007/s40264-022-01215-x
Use of Electrocardiogram Monitoring in Adult Patients Taking High-Risk QT Interval Prolonging Medicines in Clinical Practice: Systematic Review and Meta-analysis
Abstract
Introduction: Electrocardiogram (ECG) monitoring is an important tool to detect and mitigate the risk of potentially fatal drug-induced QT prolongation and remains fundamental in supporting the quality use of high-risk QT interval prolonging medicines.
Objective: The aim of this systematic review was to determine the prevalence of baseline and/or follow-up ECG use in adult patients taking high-risk QT interval prolonging medicines in clinical practice.
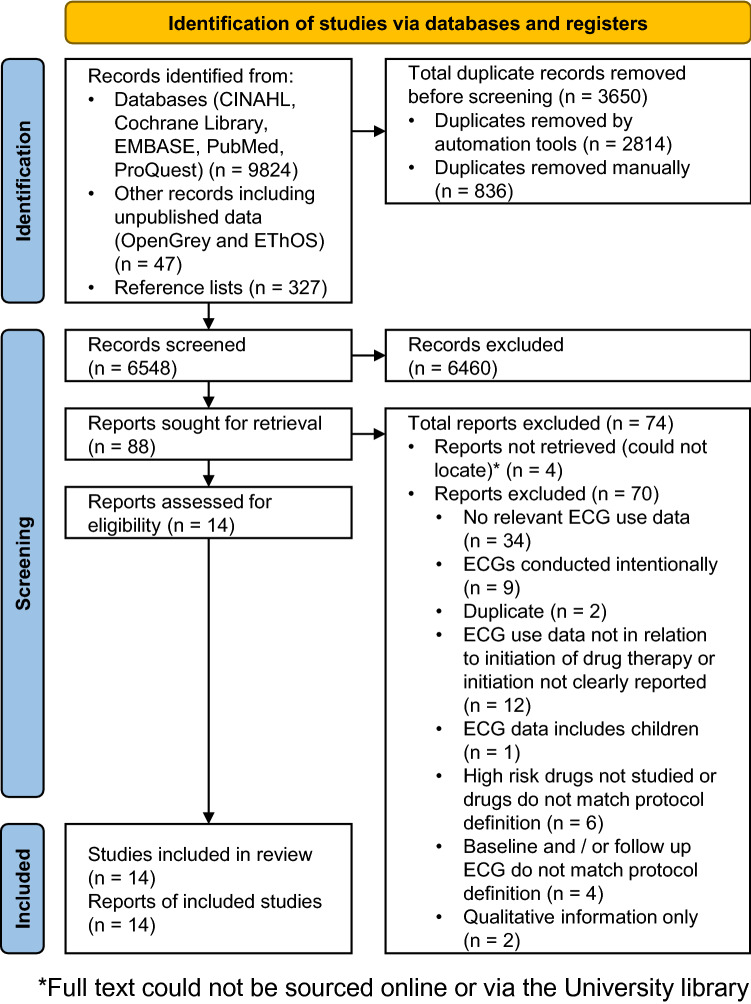
Methods: CINAHL, Cochrane Library, Embase, PubMed, EThOS, OpenGrey and Proquest were searched for studies in adults that reported ECG use at baseline and/or at follow-up in relation to the initiation of a high-risk QT interval prolonging medicine in any clinical setting; either hospital or non-hospital. Two reviewers independently assessed the methodological quality of included studies. Proportional meta-analysis was conducted with all studies reporting baseline ECG use, before medicine initiation, and follow-up ECG use, within 30 days of medicine initiation.
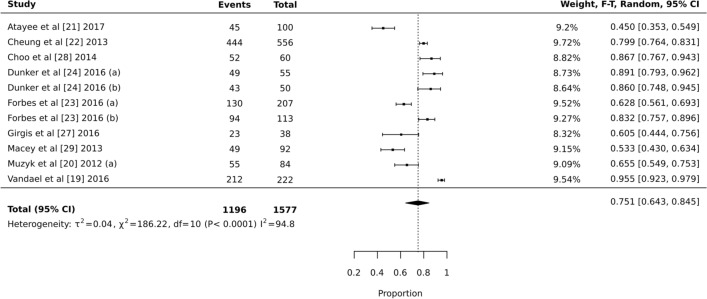
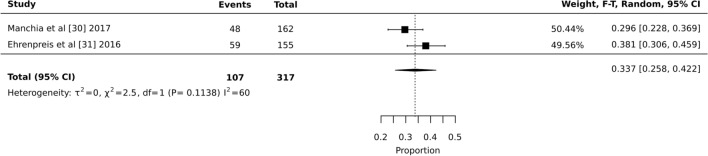
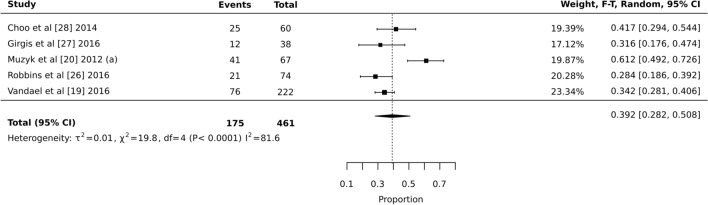
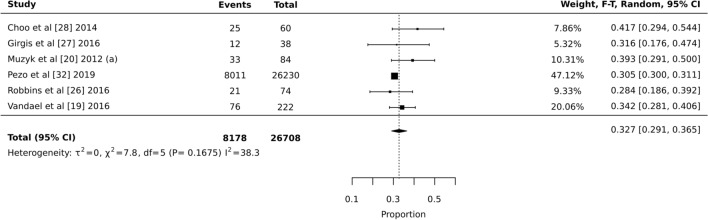
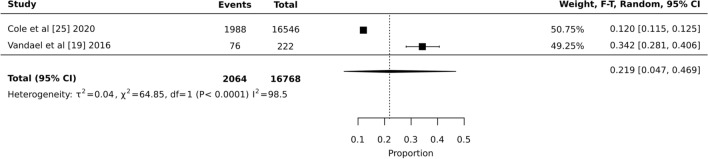
Results: There was variability in baseline ECG use according to the practice setting. The prevalence of baseline ECG use for high-risk QT interval prolonging medicines was moderate to high in the hospital setting at 75.1% (95% CI 64.3-84.5); however, the prevalence of baseline ECG use was low in the non-hospital setting at 33.7% (95% CI 25.8-42.2). The prevalence of follow-up ECG use was low to moderate in the hospital setting at 39.2% (95% CI 28.2-50.8) and could not be determined for the non-hospital setting.
Conclusions: The use of ECG monitoring for high-risk QT interval prolonging medicines is strongly influenced by the clinical practice setting. Baseline ECG use occurs more in the hospital setting in comparison to the non-hospital setting. There is lower use of follow-up ECG in comparison to baseline ECG.
© 2022. The Author(s).
Conflict of interest statement
Not applicable.
Figures
Comment in
-
Conundrum of Clinical QTc Monitoring.Drug Saf. 2022 Oct;45(10):1011-1014. doi: 10.1007/s40264-022-01229-5. Epub 2022 Aug 26. Drug Saf. 2022. PMID: 36018490 No abstract available.
Similar articles
-
Use of ECG monitoring for adult patients taking high-risk QT interval-prolonging drugs in clinical practice: a systematic review protocol.JBI Evid Synth. 2021 Nov;19(11):3113-3120. doi: 10.11124/JBIES-20-00473. JBI Evid Synth. 2021. PMID: 34054036
-
Prevalence of QT interval prolongation in patients admitted to cardiac care units and frequency of subsequent administration of QT interval-prolonging drugs: a prospective, observational study in a large urban academic medical center in the US.Drug Saf. 2012 Jun 1;35(6):459-70. doi: 10.2165/11598160-000000000-00000. Drug Saf. 2012. PMID: 22612851
-
Serial electrocardiogram recordings revealed a high prevalence of QT interval prolongation in patients with tuberculosis receiving fluoroquinolones.J Formos Med Assoc. 2023 Dec;122(12):1255-1264. doi: 10.1016/j.jfma.2023.05.020. Epub 2023 May 31. J Formos Med Assoc. 2023. PMID: 37268474
-
A review of ECG and QT interval measurement use in a public psychiatric inpatient setting.Australas Psychiatry. 2018 Feb;26(1):50-55. doi: 10.1177/1039856217726212. Epub 2017 Aug 24. Australas Psychiatry. 2018. PMID: 28836822 Review.
-
What clinicians should know about the QT interval.JAMA. 2003 Apr 23-30;289(16):2120-7. doi: 10.1001/jama.289.16.2120. JAMA. 2003. PMID: 12709470 Review.
Cited by
-
Determining sensitivity and specificity of risk scores for QTc interval prolongation in hemato-oncology patients prescribed systemic antifungal therapy: a retrospective cross-sectional study.Int J Clin Pharm. 2024 Dec;46(6):1436-1444. doi: 10.1007/s11096-024-01788-w. Epub 2024 Aug 14. Int J Clin Pharm. 2024. PMID: 39141182 Free PMC article.
-
Enhancing Cardiovascular Risk Prediction: Development of an Advanced Xgboost Model with Hospital-Level Random Effects.Bioengineering (Basel). 2024 Oct 18;11(10):1039. doi: 10.3390/bioengineering11101039. Bioengineering (Basel). 2024. PMID: 39451414 Free PMC article.
-
Conundrum of Clinical QTc Monitoring.Drug Saf. 2022 Oct;45(10):1011-1014. doi: 10.1007/s40264-022-01229-5. Epub 2022 Aug 26. Drug Saf. 2022. PMID: 36018490 No abstract available.
-
Risk Stratification of QTc Prolongations in Hospitalized Cardiology and Gastroenterology Patients Using the Tisdale Score-A Retrospective Analysis.J Clin Med. 2025 Jan 8;14(2):339. doi: 10.3390/jcm14020339. J Clin Med. 2025. PMID: 39860345 Free PMC article.
References
-
- QT interval and drug therapy. BMJ. 2016;353:i2732. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
