

Factors Influencing the Implementation of Prone Positioning during the COVID-19 Pandemic: A Qualitative Study
- PMID: 35947776
- PMCID: PMC9819268
- DOI: 10.1513/AnnalsATS.202204-349OC
Factors Influencing the Implementation of Prone Positioning during the COVID-19 Pandemic: A Qualitative Study
Abstract
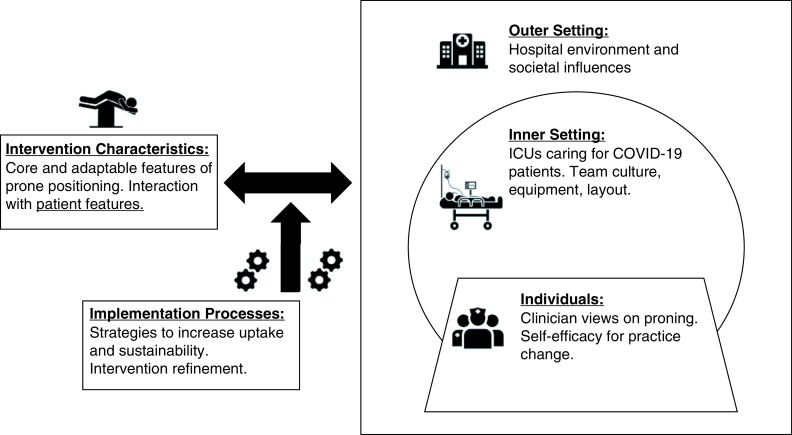
Rationale: The adoption of prone positioning for patients with acute respiratory distress syndrome (ARDS) has historically been poor. However, in mechanically ventilated patients with coronavirus disease (COVID-19) ARDS, proning has increased. Understanding the factors influencing this change is important for further expanding and sustaining the use of prone positioning in appropriate clinical settings. Objectives: To characterize factors influencing the implementation of prone positioning in mechanically ventilated patients with COVID-19 ARDS. Methods: We conducted a qualitative study using semistructured interviews with 40 intensive care unit (ICU) team members (physicians, nurses, advanced practice providers, respiratory therapists, and physical therapists) working at two academic hospitals. We used the Consolidated Framework for Implementation Research, a widely used implementation science framework outlining important features of implementation, to structure the interview guide and thematic analysis of interviews. Results: ICU clinicians reported that during the COVID-19 pandemic, proning was viewed as standard early therapy for COVID-19 ARDS rather than salvage therapy for refractory hypoxemia. By caring for large volumes of proned patients, clinicians gained increased comfort with proning and now view proning as a low-risk, high-benefit intervention. Within ICUs, adequate numbers of trained staff members, increased team agreement around proning, and the availability of specific equipment (e.g., to limit pressure injuries) facilitated greater proning use. Hospital-level supports included proning teams, centralized educational resources specific to the management of COVID-19 (including a recommendation for prone positioning), and an electronic medical record proning order. Important implementation processes included informal dissemination of best practices through on-the-job learning and team interactions during routine bedside care. Conclusions: The implementation of prone positioning for COVID-19 ARDS took place in the context of evolving clinician viewpoints and ICU team cultures. Proning was facilitated by hospital support and buy-in and leadership from bedside clinicians. The successful implementation of prone positioning during the COVID-19 pandemic may serve as a model for the implementation of other evidence-based therapies in critical care.
Keywords: acute respiratory distress syndrome; coronavirus disease; implementation science; prone positioning.
Figures
Similar articles
-
Adaptation and Uncertainty: A Qualitative Examination of Provider Experiences With Prone Positioning for Intubated Patients With COVID-19 ARDS.CHEST Crit Care. 2023 Sep;1(2):100008. doi: 10.1016/j.chstcc.2023.100008. Epub 2023 Jun 30. CHEST Crit Care. 2023. PMID: 37810258 Free PMC article.
-
Improving Prone Positioning for Severe Acute Respiratory Distress Syndrome during the COVID-19 Pandemic. An Implementation-Mapping Approach.Ann Am Thorac Soc. 2021 Feb;18(2):300-307. doi: 10.1513/AnnalsATS.202005-571OC. Ann Am Thorac Soc. 2021. PMID: 33522870 Free PMC article.
-
Comparing Prone Positioning Use in COVID-19 Versus Historic Acute Respiratory Distress Syndrome.Crit Care Explor. 2022 May 13;4(5):e0695. doi: 10.1097/CCE.0000000000000695. eCollection 2022 May. Crit Care Explor. 2022. PMID: 35783548 Free PMC article.
-
Prone Positioning for Acute Hypoxemic Respiratory Failure and ARDS: A Review.Chest. 2023 Feb;163(2):332-340. doi: 10.1016/j.chest.2022.09.020. Epub 2022 Sep 23. Chest. 2023. PMID: 36162482 Review.
-
Proning Patients With COVID-19: A Review of Equipment and Methods.Hum Factors. 2020 Nov;62(7):1069-1076. doi: 10.1177/0018720820950532. Epub 2020 Aug 16. Hum Factors. 2020. PMID: 32845730 Free PMC article. Review.
Cited by
-
Declining Use of Prone Positioning After High Initial Uptake in COVID-19 Adult Respiratory Distress Syndrome.Crit Care Med. 2023 Nov 1;51(11):1547-1551. doi: 10.1097/CCM.0000000000005969. Epub 2023 Jun 9. Crit Care Med. 2023. PMID: 37294144 Free PMC article.
-
Barriers and facilitators of adherence to awake prone positioning: a qualitative study using the COM-B model.BMC Pulm Med. 2023 Jul 19;23(1):267. doi: 10.1186/s12890-023-02561-x. BMC Pulm Med. 2023. PMID: 37468848 Free PMC article.
-
Adaptation and Uncertainty: A Qualitative Examination of Provider Experiences With Prone Positioning for Intubated Patients With COVID-19 ARDS.CHEST Crit Care. 2023 Sep;1(2):100008. doi: 10.1016/j.chstcc.2023.100008. Epub 2023 Jun 30. CHEST Crit Care. 2023. PMID: 37810258 Free PMC article.
-
Outcomes of Patients Transported in the Prone Position to a Regional Extracorporeal Membrane Oxygenation Center: A Retrospective Cohort Study.Crit Care Explor. 2023 Jul 21;5(7):e0948. doi: 10.1097/CCE.0000000000000948. eCollection 2023 Jul. Crit Care Explor. 2023. PMID: 37492857 Free PMC article.
-
A Comprehensive Review of Prone Ventilation in the Intensive Care Unit: Challenges and Solutions.Cureus. 2024 Mar 30;16(3):e57247. doi: 10.7759/cureus.57247. eCollection 2024 Mar. Cureus. 2024. PMID: 38686225 Free PMC article. Review.
References
-
- Guérin C, Reignier J, Richard J-C, Beuret P, Gacouin A, Boulain T, et al. PROSEVA Study Group Prone positioning in severe acute respiratory distress syndrome. N Engl J Med . 2013;368:2159–2168. - PubMed
-
- Munshi L, Del Sorbo L, Adhikari NKJ, Hodgson CL, Wunsch H, Meade MO, et al. Prone position for acute respiratory distress syndrome: a systematic review and meta-analysis. Ann Am Thorac Soc . 2017;14:S280–S288. - PubMed
-
- Sud S, Friedrich JO, Adhikari NKJ, Fan E, Ferguson ND, Guyatt G, et al. Comparative effectiveness of protective ventilation strategies for moderate and severe acute respiratory distress syndrome: a network meta-analysis. Am J Respir Crit Care Med . 2021;203:1366–1377. - PubMed
-
- Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, et al. American Thoracic Society, European Society of Intensive Care Medicine, and Society of Critical Care Medicine An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med . 2017;195:1253–1263. - PubMed
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. LUNG SAFE Investigators ESICM Trials Group. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA . 2016;315:788–800. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
