

Cost-effectiveness and sustainability of improved hospital oxygen systems in Nigeria
- PMID: 35948344
- PMCID: PMC9379491
- DOI: 10.1136/bmjgh-2022-009278
Cost-effectiveness and sustainability of improved hospital oxygen systems in Nigeria
Abstract
Introduction: Improving hospital oxygen systems can improve quality of care and reduce mortality for children, but we lack data on cost-effectiveness or sustainability. This study evaluated medium-term sustainability and cost-effectiveness of the Nigeria Oxygen Implementation programme.
Methods: Prospective follow-up of a stepped-wedge trial involving 12 secondary-level hospitals. Cross-sectional facility assessment, clinical audit (January-March 2021), summary admission data (January 2018-December 2020), programme cost data.
Intervention: pulse oximetry introduction followed by solar-powered oxygen system installation with clinical and technical training and support.
Primary outcomes: (i) proportion of children screened with pulse oximetry; (ii) proportion of hypoxaemic (SpO2 <90%) children who received oxygen. Comparison across three time periods: preintervention (2014-2015), intervention (2016-2017) and follow-up (2018-2020) using mixed-effects logistic regression. Calculated cost-effectiveness of the intervention on child pneumonia mortality using programme costs, recorded deaths and estimated counterfactual deaths using effectiveness estimates from our effectiveness study. Reported cost-effectiveness over the original 2-year intervention period (2016-2017) and extrapolated over 5 years (2016-2020).
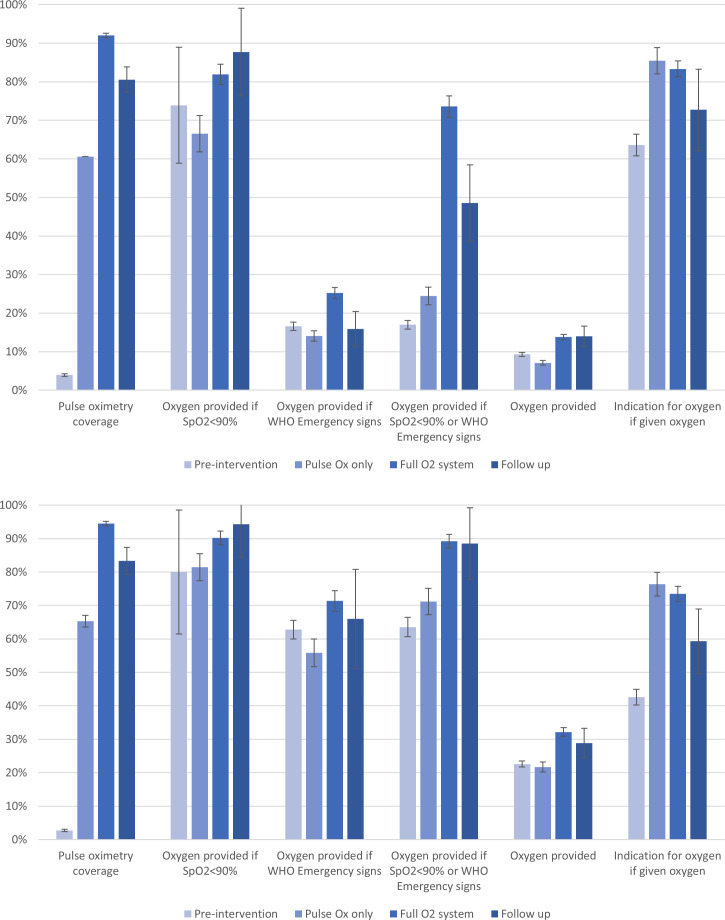
Results: Pulse oximetry coverage for neonates and children remained high during follow-up (83% and 81%) compared with full oxygen system period (94% and 92%) and preintervention (3.9% and 2.9%). Oxygen coverage for hypoxaemic neonates/children was similarly high (94%/88%) compared with full oxygen system period (90%/82%). Functional oxygen sources were present in 11/12 (92%) paediatric areas and all (8/8) neonatal areas; three-quarters (15/20) of wards had a functional oximeter. Of 32 concentrators deployed, 23/32 (72%) passed technical testing and usage was high (median 10 797 hours). Estimated 5-year cost-effectiveness US$86 per patient treated, $2694-4382 per life saved and $82-125 per disability-adjusted life year-averted. We identified practical issues for hospitals and Ministries of Health wishing to adapt and scale up pulse oximetry and oxygen.
Conclusion: Hospital-level improvements to oxygen and pulse oximetry systems in Nigerian hospitals have been sustained over the medium-term and are a highly cost-effective child pneumonia intervention.
Keywords: Child health; Health economics; Health services research; Paediatrics; Pneumonia.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- ed.:.WHO . Pocket Book of Hospital care for children: guidelines for the management of common childhood illnesses.. In: 2Nd. Geneva: World Health Organization, 2013. - PubMed
-
- WHO . Standards for improving the quality of care for children and young adolescents in health facilities. Geneva: World Health Organization, 2018.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical