

Outcome disparities in patients with atrial fibrillation based on insurance plan and educational attainment: a nationwide, multicenter and prospective cohort trial
- PMID: 35948379
- PMCID: PMC9379473
- DOI: 10.1136/bmjopen-2021-053166
Outcome disparities in patients with atrial fibrillation based on insurance plan and educational attainment: a nationwide, multicenter and prospective cohort trial
Abstract
Background: Atrial fibrillation (AF) is a complex disease. The management of AF requires continuous patient engagement and integrative healthcare.
Objectives: To explore the association between adverse AF-related clinical outcomes and the following two sociodemographic factors: educational attainment and insurance plan.
Design: A nationwide, prospective, multicenter, cohort trial.
Setting: National registry of 3402 patients with non-valvular AF in Thailand.
Participants: All patients enrolled in the registry, except those with missing information on educational attainment or insurance plan. Finally, data from 3026 patients (mean age 67 years, SD 11.3; 59% male sex) were analysed.
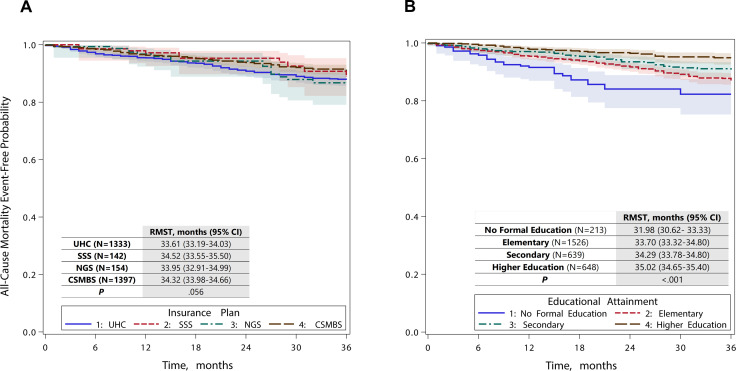
Primary outcomes: Incidences of all-cause mortality, ischaemic stroke and major bleeding during the 36-month follow-up period. Survival analysis was performed using restricted mean survival time (RMST) and adjusted for multiple covariates. The levels of the educational attainment were as follows: no formal education, elementary (grade 1-6), secondary (grade 7-12) and higher education (tertiary education).
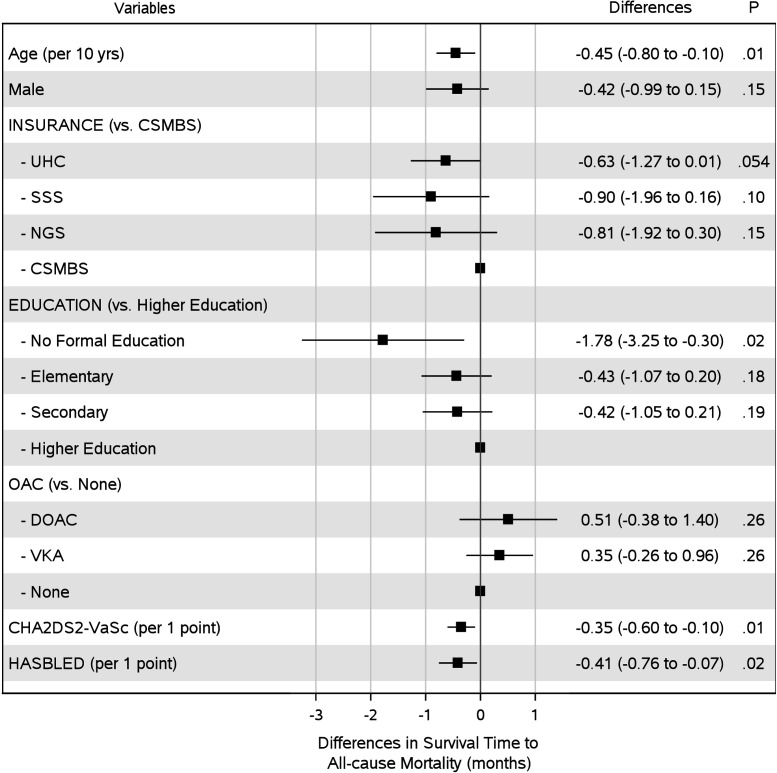
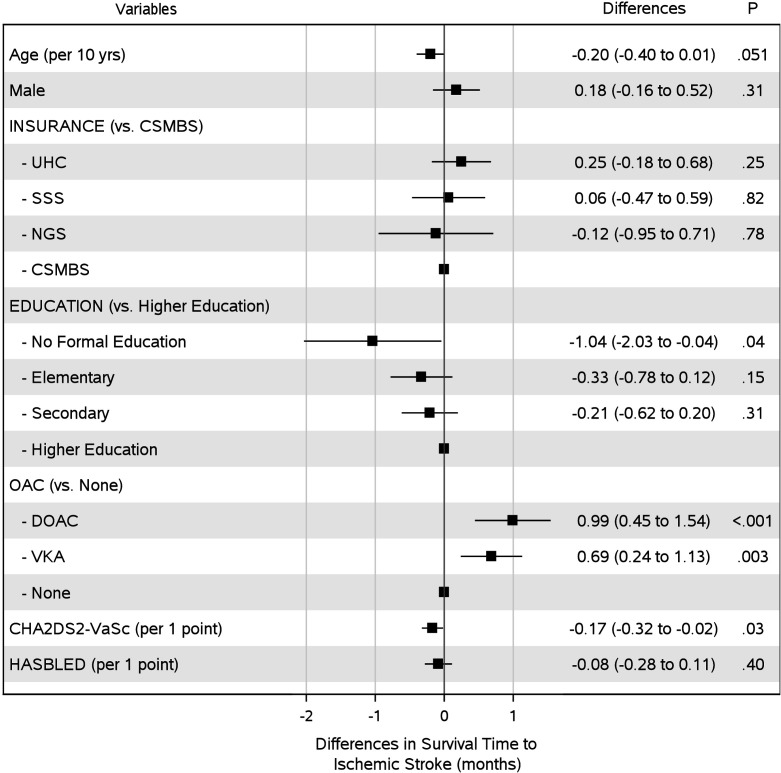
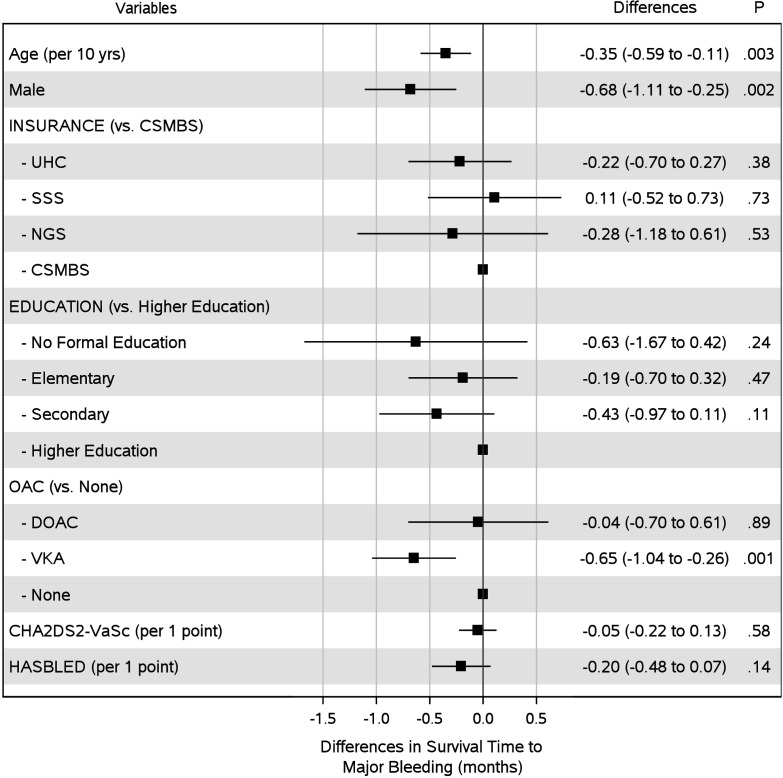
Results: The educational attainment of the majority of patients was elementary (N=1739, 57.4%). The predominant health insurance plans were the Civil Servant Medical Benefit Scheme (N=1397, 46.2%) and the Universal Coverage Scheme (N=1333, 44.1%). After 36 months of follow-up, 248 patients died (8.2%), 95 had ischaemic stroke (3.1%) and 136 had major bleeding (4.5%). Patients without formal education died 1.78 months earlier (adjusted RMST difference -1.78; 95% CI, -3.25 to -0.30; p=0.02) and developed ischaemic stroke 1.04 months sooner (adjusted RMST difference -1.04; 95% CI, -2.03 to -0.04; p=0.04) than those attained a level of higher education. There were no significant differences in RMSTs for all three clinical outcomes when considering the type of health insurance plan.
Conclusion: Educational attainment was independently associated with all-cause mortality and ischaemic stroke in patients with AF, but adverse clinical outcomes were not related to the types of health insurance in Thailand.
Trial registration number: Thai Clinical Trial Registration; Study ID: TCTR20160113002.
Keywords: Adult cardiology; Health policy; PUBLIC HEALTH; Thromboembolism.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- James C, Devaux M, Sassi F. "Inclusive growth and health", OECD Health Working Papers, No. 103. Paris: OECD Publishing, 2017.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical