

The prognosis of non-small cell lung cancer patients according to endobronchial metastatic lesion
- PMID: 35948652
- PMCID: PMC9365769
- DOI: 10.1038/s41598-022-17918-1
The prognosis of non-small cell lung cancer patients according to endobronchial metastatic lesion
Abstract
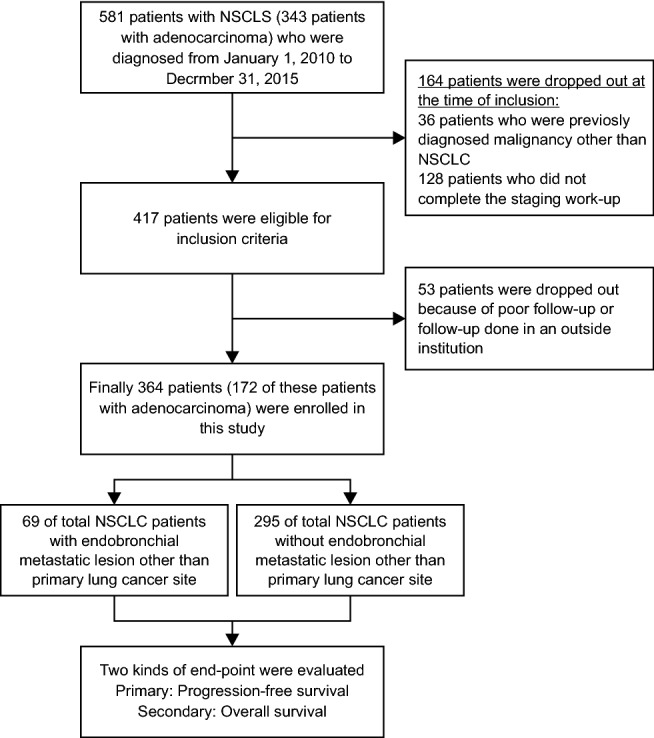
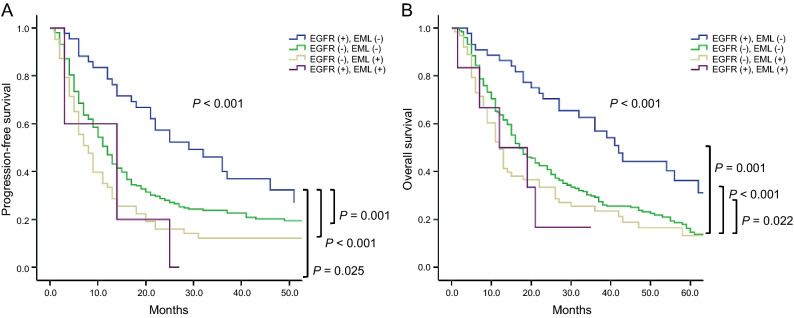
To evaluate the prognosis of non-small cell lung cancer (NSCLC) patients according to endobronchial metastatic lesion (EML), especially those not identified on positron emission tomography or computed tomography. We evaluated progression-free survival (PFS) and overall survival (OS) according to the presence of EML in patients with NSCLC who were diagnosed at a tertiary hospital between January 2010 and December 2019. A total of 364 patients were enrolled in this study. EML was found in 69 (19.0%) patients with NSCLC. In the patients with EML versus the patients without EML, median PFS was 7.0 (3.5-13.5) and 9.5 (5.5-17.5) months (P = 0.011), and median OS was 12.0 (6.0-30.0) versus 20.0 (10.0-39.0) months (P = 0.016), respectively. Median PFS and OS rates were highest in epidermal growth factor receptor (EGFR) (+) and EML (-) patients and lowest in EGFR (-) and EML (+) patients (P < 0.001). By multivariate cox regression analysis, PFS in overall patients with NSCLC was significantly associated with EML, EGFR mutation, performance status, and pleural effusion. NSCLC patients with EML had worse prognoses of PFS and OS than patients without EML.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Silvestri GA, Hoffman B, Reed CE. One from column A: choosing between CT, positron emission tomography, endoscopic ultrasound with fine-needle aspiration, transbronchial needle aspiration, thoracoscopy, mediastinoscopy, and mediastinotomy for staging lung cancer. Chest. 2003;123(2):333–335. doi: 10.1378/chest.123.2.333. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
