

Analysis in the influence factors of urethroplasty in DSD
- PMID: 35948888
- PMCID: PMC9367162
- DOI: 10.1186/s12894-022-01080-x
Analysis in the influence factors of urethroplasty in DSD
Abstract
Background: At present, there is no specific research on the factors affecting the success rate of urethroplasty in patients with DSD. The purpose of this study is to explore the factors affecting the success of urethroplasty in DSD patients, and to provide some reference for the surgical treatment of DSD patients undergoing urethroplasty.
Method: We reviewed patients with DSD who underwent urethroplasty from January 2016 to December 2019 retrospectively. Patients were divided into four groups: the successful group, the urethrocutaneous fistula group, the urethral diverticulum group, and the urethral stricture group. Risk factors were determined from the following data included the DSD classification, the age of first operation, length of urethral defect, degree of hypospadias, cryptorchidism, micropenis, gonad type, hormone therapy before operation, transposition of penis and scrotum, surgical strategy, urethral covering material, and postoperative catheter removal time. We explored the difference of each factor between four groups through the comparative study of single factor and multifactor logistic regression analysis of related factors.
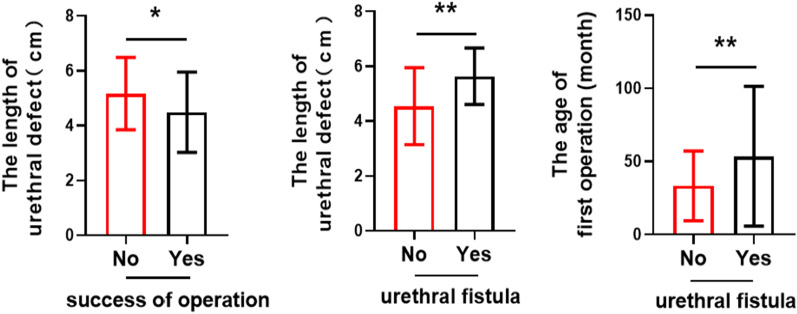
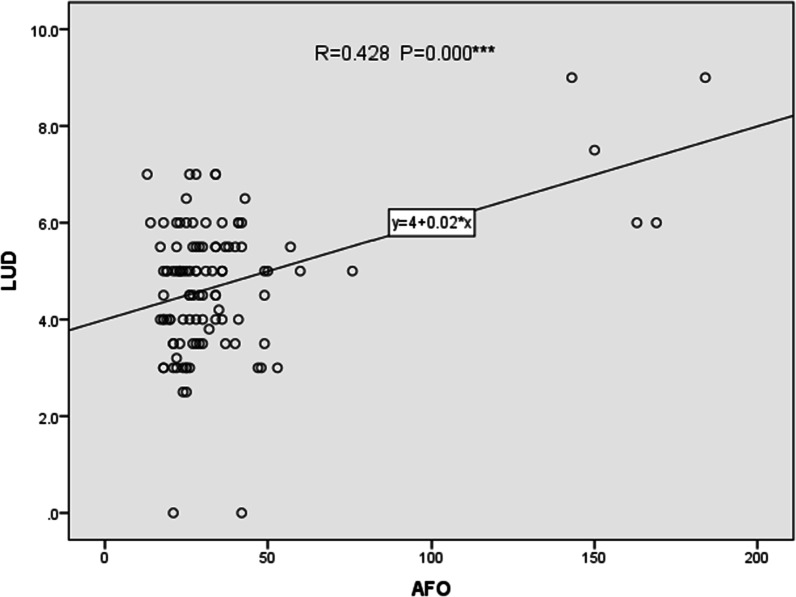
Result: 122 cases were enrolled in this group (n = 122), 12 cases were lost to follow-up. Median follow-up was 28 months (12-55 months).We found the success rate of operation decreased with longer urethral defect (B = - 0.473, P = 0.005). The success rate of operation was higher in staged operation and TPIT (TPIT = Transverse Preputial Island Tube operation)-related operation than primary operation (B = 1.238, P = 0.006) and TPIT-nonrelated operation (B = 2.293, P = 0.001). Although there was a significant difference between the age of the first operation and the occurrence of urethrocutaneous fistula (P = 0.006 < 0.05), there was no significant difference in logistic regression analysis (P = 0.161 > 0.05). The incidence of urethrocutaneous fistula was lower in TPIT-related operation than in TPIT-nonrelated operation (B = - 2.507, P = 0.000). The incidence of postoperative urethral diverticulum was lower in staged operation than in primary operation (B = - 1.737, P = 0.015).
Conclusion: For patients with disorder of sex development undergoing urethroplasty, the length of urethral defect is an independent risk factor affecting both the success rate of operation and the urethrocutaneous fistula. The age of the first operation has a statistically significant effect on the occurrence of postoperative urethrocutaneous fistula, but it is not an independent factor. Urethrocutaneous fistula is less found in TPIT-related operation in the study. Staged operation is an independent protective factor for postoperative urethral diverticulum compared with one-stage operation but isn't related to urethrocutaneous fistula.
Keywords: Analysis; Disorders of sex development; Influencing factors; Urethroplasty.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Tang D, Fu J. New understanding and surgical choice of DSD. Chin J Pediatic Surg. 2016;37(7):481–484.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
