

An inline deep learning based free-breathing ECG-free cine for exercise cardiovascular magnetic resonance
- PMID: 35948936
- PMCID: PMC9367083
- DOI: 10.1186/s12968-022-00879-9
An inline deep learning based free-breathing ECG-free cine for exercise cardiovascular magnetic resonance
Abstract
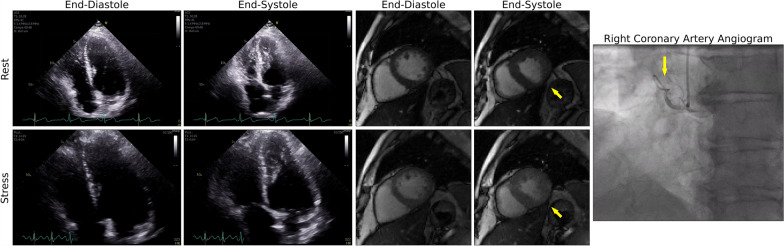
Background: Exercise cardiovascular magnetic resonance (Ex-CMR) is a promising stress imaging test for coronary artery disease (CAD). However, Ex-CMR requires accelerated imaging techniques that result in significant aliasing artifacts. Our goal was to develop and evaluate a free-breathing and electrocardiogram (ECG)-free real-time cine with deep learning (DL)-based radial acceleration for Ex-CMR.
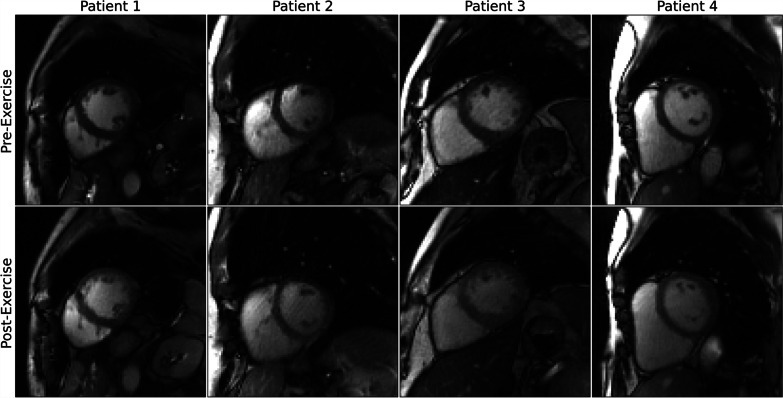
Methods: A 3D (2D + time) convolutional neural network was implemented to suppress artifacts from aliased radial cine images. The network was trained using synthetic real-time radial cine images simulated using breath-hold, ECG-gated segmented Cartesian k-space data acquired at 3 T from 503 patients at rest. A prototype real-time radial sequence with acceleration rate = 12 was used to collect images with inline DL reconstruction. Performance was evaluated in 8 healthy subjects in whom only rest images were collected. Subsequently, 14 subjects (6 healthy and 8 patients with suspected CAD) were prospectively recruited for an Ex-CMR to evaluate image quality. At rest (n = 22), standard breath-hold ECG-gated Cartesian segmented cine and free-breathing ECG-free real-time radial cine images were acquired. During post-exercise stress (n = 14), only real-time radial cine images were acquired. Three readers evaluated residual artifact level in all collected images on a 4-point Likert scale (1-non-diagnostic, 2-severe, 3-moderate, 4-minimal).
Results: The DL model substantially suppressed artifacts in real-time radial cine images acquired at rest and during post-exercise stress. In real-time images at rest, 89.4% of scores were moderate to minimal. The mean score was 3.3 ± 0.7, representing increased (P < 0.001) artifacts compared to standard cine (3.9 ± 0.3). In real-time images during post-exercise stress, 84.6% of scores were moderate to minimal, and the mean artifact level score was 3.1 ± 0.6. Comparison of left-ventricular (LV) measures derived from standard and real-time cine at rest showed differences in LV end-diastolic volume (3.0 mL [- 11.7, 17.8], P = 0.320) that were not significantly different from zero. Differences in measures of LV end-systolic volume (7.0 mL [- 1.3, 15.3], P < 0.001) and LV ejection fraction (- 5.0% [- 11.1, 1.0], P < 0.001) were significant. Total inline reconstruction time of real-time radial images was 16.6 ms per frame.
Conclusions: Our proof-of-concept study demonstrated the feasibility of inline real-time cine with DL-based radial acceleration for Ex-CMR.
Keywords: Coronary artery disease; Deep learning; Exercise MRI; Inline; Radial golden angle.
© 2022. The Author(s).
Conflict of interest statement
Xiaoying Cai and Kelvin Chow are employees of Siemens Medical Solutions USA, Inc. Reza Nezafat has a research agreement with Siemens. Hassan Haji-valizadeh is an employee of Canon Medical Research USA, Inc.
Figures







Similar articles
-
Free-breathing single-beat exercise cardiovascular magnetic resonance with generative artificial intelligence for evaluation of volumetric and functional cardiac indices: A reproducibility study.J Cardiovasc Magn Reson. 2025 Summer;27(1):101901. doi: 10.1016/j.jocmr.2025.101901. Epub 2025 Apr 30. J Cardiovasc Magn Reson. 2025. PMID: 40316174 Free PMC article.
-
Accelerated Cardiac MRI Cine with Use of Resolution Enhancement Generative Adversarial Inline Neural Network.Radiology. 2023 Jun;307(5):e222878. doi: 10.1148/radiol.222878. Radiology. 2023. PMID: 37249435 Free PMC article.
-
Highly accelerated free-breathing real-time myocardial tagging for exercise cardiovascular magnetic resonance.J Cardiovasc Magn Reson. 2023 Oct 2;25(1):56. doi: 10.1186/s12968-023-00961-w. J Cardiovasc Magn Reson. 2023. PMID: 37784153 Free PMC article.
-
Artifacts at Cardiac MRI: Imaging Appearances and Solutions.Radiographics. 2025 Jan;45(1):e230200. doi: 10.1148/rg.230200. Radiographics. 2025. PMID: 39745866 Review.
-
Reconstruction techniques for accelerating dynamic cardiovascular magnetic resonance imaging.J Cardiovasc Magn Reson. 2025 Summer;27(1):101873. doi: 10.1016/j.jocmr.2025.101873. Epub 2025 Mar 6. J Cardiovasc Magn Reson. 2025. PMID: 40057040 Free PMC article. Review.
Cited by
-
Accelerated real-time cine and flow under in-magnet staged exercise.J Cardiovasc Magn Reson. 2025 Summer;27(1):101894. doi: 10.1016/j.jocmr.2025.101894. Epub 2025 Apr 10. J Cardiovasc Magn Reson. 2025. PMID: 40220901 Free PMC article.
-
Physical exercise and cardiovascular response: design and implementation of a pediatric CMR cohort study.Int J Cardiovasc Imaging. 2023 Dec;39(12):2575-2587. doi: 10.1007/s10554-023-02950-7. Epub 2023 Oct 6. Int J Cardiovasc Imaging. 2023. PMID: 37801171 Free PMC article.
-
A low-rank deep image prior reconstruction for free-breathing ungated spiral functional CMR at 0.55 T and 1.5 T.MAGMA. 2023 Jul;36(3):451-464. doi: 10.1007/s10334-023-01088-w. Epub 2023 Apr 12. MAGMA. 2023. PMID: 37043121 Free PMC article.
-
Free-breathing single-beat exercise cardiovascular magnetic resonance with generative artificial intelligence for evaluation of volumetric and functional cardiac indices: A reproducibility study.J Cardiovasc Magn Reson. 2025 Summer;27(1):101901. doi: 10.1016/j.jocmr.2025.101901. Epub 2025 Apr 30. J Cardiovasc Magn Reson. 2025. PMID: 40316174 Free PMC article.
-
Stop moving: MR motion correction as an opportunity for artificial intelligence.MAGMA. 2024 Jul;37(3):397-409. doi: 10.1007/s10334-023-01144-5. Epub 2024 Feb 22. MAGMA. 2024. PMID: 38386151 Review.
References
-
- Members WC, Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER, Beckie TM, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;79(2):e21–e129. doi: 10.1016/j.jacc.2021.09.006. - DOI - PubMed
-
- Schwitter J, Wacker CM, Wilke N, Al-Saadi N, Sauer E, Huettle K, et al. MR-IMPACT II: Magnetic Resonance Imaging for Myocardial Perfusion Assessment in Coronary artery disease Trial: perfusion-cardiac magnetic resonance vs. single-photon emission computed tomography for the detection of coronary artery disease: a comparative multicentre, multivendor trial. Eur Heart J. 2013;34(10):775–781. doi: 10.1093/eurheartj/ehs022. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
