

A process evaluation of 'We Can Quit': a community-based smoking cessation intervention targeting women from areas of socio-disadvantage in Ireland
- PMID: 35948970
- PMCID: PMC9367164
- DOI: 10.1186/s12889-022-13957-5
A process evaluation of 'We Can Quit': a community-based smoking cessation intervention targeting women from areas of socio-disadvantage in Ireland
Abstract
Background: Smoking poses a serious risk of early preventable death and disease especially for women living with socio-economic disadvantage (SED). A smoking cessation programme, 'We Can Quit', was developed in Ireland tailored to SED women. This includes group-based support delivered by trained lay local community facilitators (CFs) and free nicotine replacement therapy (NRT). The intervention was pilot tested in a cluster randomised controlled trial, 'We Can Quit 2'. This paper reports on the WCQ2 process evaluation which assessed feasibility and acceptability of the programme and trial processes.
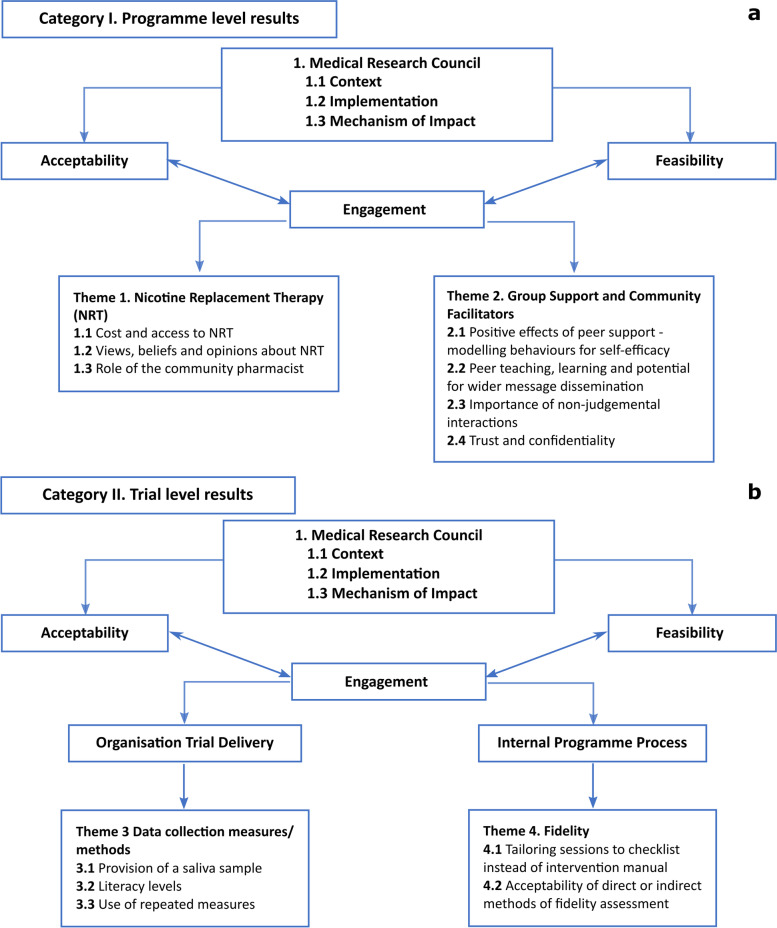
Methods: Embedded qualitative design using the UK Medical Research Council's process evaluation framework. Semi-structured interviews with trial participants (N = 21) and CFs (N = 8). Thematic analysis was utilised.
Results: Peer-modelling, a non-judgemental environment, CFs facilitation of group support were viewed as acceptable programme related factors. Some participants expressed concerns about NRT side effects. Provision of free NRT was welcomed and accepted by participants, although structural barriers made access challenging. Pharmacists took on a role that became larger than originally envisaged - and the majority provided additional support to women in their quit attempts between group meetings which augmented and supplemented the intervention sessions provided by the CFs. Participants reported good acceptance of repeated measures for data collection, but mixed acceptability of provision of saliva samples. Low literacy affected the feasibility of some women to fully engage with programme and trial-related materials. This was despite efforts made by intervention developers and the trial team to make materials (e.g., participant intervention booklet; consent forms and participant information leaflets) accessible while also meeting requirements under 2018 European General Data Protection Regulation legislation. Hypothetical scenarios of direct (e.g., researcher present during programme delivery) and indirect (e.g., audio recordings of programme sessions) observational fidelity assessments for a future definitive trial (DT) were acceptable.
Conclusions: Intervention and trial-related processes were generally feasible and acceptable to participants and CFs. Any future DT will need to take further steps to mitigate structural barriers to accessing free NRT; and the established problem of low literacy and low educational attainment in SED areas, while continuing to comply within the contemporary legislative research environment.
Trial registration: WCQ2 pilot trial ( ISRCTN74721694 ).
Keywords: Behavioural intervention; Deprivation; NRT; Process evaluation; Qualitative; Smoking cessation; Trials; Women.
© 2022. The Author(s).
Conflict of interest statement
CBH reports grants from HRB and Enterprise Ireland during the conduct of the study. CD reports grants from HRB during the conduct of the study. All the remaining authors do not have any competing interests.
Figures
Similar articles
-
We Can Quit2 (WCQ2): a community-based intervention on smoking cessation for women living in disadvantaged areas of Ireland-study protocol for a pilot cluster randomised controlled trial.Pilot Feasibility Stud. 2019 Nov 23;5:138. doi: 10.1186/s40814-019-0511-9. eCollection 2019. Pilot Feasibility Stud. 2019. PMID: 31788324 Free PMC article.
-
Peer-Delivery of a Gender-Specific Smoking Cessation Intervention for Women Living in Disadvantaged Communities in Ireland We Can Quit2 (WCQ2)-A Pilot Cluster Randomized Controlled Trial.Nicotine Tob Res. 2022 Mar 1;24(4):564-573. doi: 10.1093/ntr/ntab242. Nicotine Tob Res. 2022. PMID: 34939119 Free PMC article. Clinical Trial.
-
A pilot cluster randomised controlled trial of a peer-delivered outreach community-based smoking cessation intervention for women living in disadvantaged communities in Ireland.Rural Remote Health. 2023 Jan;23(1):8163. doi: 10.22605/RRH8163. Epub 2023 Jan 10. Rural Remote Health. 2023. PMID: 36802719 Clinical Trial.
-
Different doses, durations and modes of delivery of nicotine replacement therapy for smoking cessation.Cochrane Database Syst Rev. 2019 Apr 18;4(4):CD013308. doi: 10.1002/14651858.CD013308. Cochrane Database Syst Rev. 2019. Update in: Cochrane Database Syst Rev. 2023 Jun 19;6:CD013308. doi: 10.1002/14651858.CD013308.pub2. PMID: 30997928 Free PMC article. Updated.
-
Factors influencing the uptake and use of nicotine replacement therapy and e-cigarettes in pregnant women who smoke: a qualitative evidence synthesis.Cochrane Database Syst Rev. 2020 May 22;5(5):CD013629. doi: 10.1002/14651858.CD013629. Cochrane Database Syst Rev. 2020. PMID: 32441810 Free PMC article.
Cited by
-
The We Can Quit2 Smoking Cessation Trial: Knowledge Exchange and Dissemination Following a Community-Based Participatory Research Approach.Int J Environ Res Public Health. 2022 Feb 18;19(4):2333. doi: 10.3390/ijerph19042333. Int J Environ Res Public Health. 2022. PMID: 35206521 Free PMC article. Clinical Trial.
-
Health behavior interventions among people with lower socio-economic position: a scoping review of behavior change techniques and effectiveness.Health Psychol Behav Med. 2024 Jun 18;12(1):2365931. doi: 10.1080/21642850.2024.2365931. eCollection 2024. Health Psychol Behav Med. 2024. PMID: 38903803 Free PMC article.
-
How can engagement with underserved communities be enhanced? A co-inquiry informed model of stop smoking outreach.Perspect Public Health. 2025 Mar;145(2):97-104. doi: 10.1177/17579139251322314. Epub 2025 Mar 31. Perspect Public Health. 2025. PMID: 40165409 Free PMC article.
-
Evaluating the implementation of adult smoking cessation programs in community settings: a scoping review.Front Public Health. 2025 Mar 28;12:1495151. doi: 10.3389/fpubh.2024.1495151. eCollection 2024. Front Public Health. 2025. PMID: 40225818 Free PMC article.
-
Barriers to smoking interventions in community healthcare settings: a scoping review.Health Promot Int. 2024 Apr 1;39(2):daae036. doi: 10.1093/heapro/daae036. Health Promot Int. 2024. PMID: 38666785 Free PMC article.
References
-
- World Health Organization. European Tobacco Use. Trends Report 2019 [Internet]. Geneva, Switzerland: WHO; 2019 [cited 2021 Mar 24]. Available from: https://www.euro.who.int/__data/assets/pdf_file/0009/402777/Tobacco-Tren...
-
- World Health Organization. Guidelines for implementation of Article 14. Guidelines on demand reduction measures concerning tobacco dependence and cessation. [Internet]. Geneva, Switzerland: WHO; 2010 [cited 2021 Mar 24]. (WHO Framework Convention on Tobacco Control). Available from: https://www.who.int/fctc/guidelines/adopted/article_14/en/
-
- Walsh PM, McDevitt J, Deady S, O’Brien K, Comber H. Cancer inequalities in Ireland by deprivation, urban/rural status and age: a report by the National Cancer Registry. [Internet]. Cork, Ireland: National Cancer Registry; 2016 [cited 2021 Mar 24]. Available from: https://www.ncri.ie/sites/ncri/files/pubs/cancer-inequality-report-summa...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
