

COVID-19 and Acute Neurologic Complications in Children
- PMID: 35949041
- PMCID: PMC9633383
- DOI: 10.1542/peds.2022-058167
COVID-19 and Acute Neurologic Complications in Children
Abstract
Background: Little is known about the epidemiology and outcomes of neurologic complications associated with coronavirus disease 2019 (COVID-19) in children.
Methods: We performed a cross-sectional study of children 2 months to <18 years of age with COVID-19 discharged from 52 children's hospitals from March 2020 to March 2022. Neurologic complications were defined as encephalopathy, encephalitis, aseptic meningitis, febrile seizure, nonfebrile seizure, brain abscess and bacterial meningitis, Reye's syndrome, and cerebral infarction. We assessed length of stay (LOS), ICU admission, 30 day readmissions, deaths, and hospital costs. We used multivariable logistic regression to identify factors associated with neurologic complications.
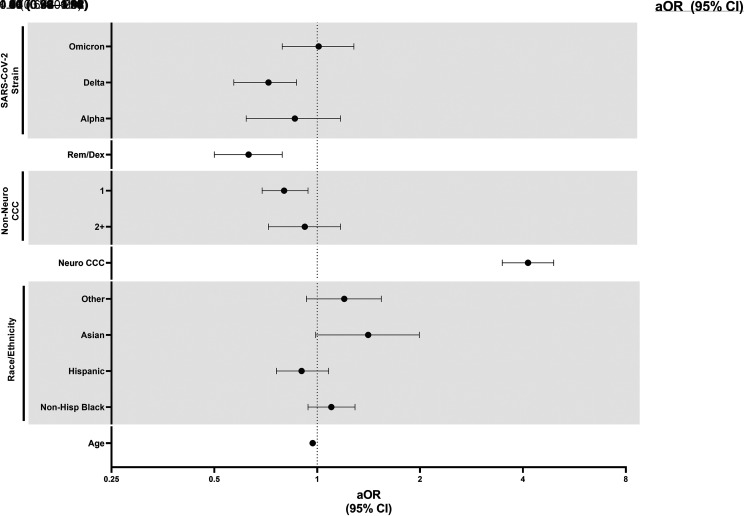
Results: Of 15 137 children hospitalized with COVID-19, 1060 (7.0%) had a concurrent diagnosis of a neurologic complication. The most frequent neurologic complications were febrile seizures (3.9%), nonfebrile seizures (2.3%), and encephalopathy (2.2%). Hospital LOS, ICU admission, ICU LOS, 30 day readmissions, deaths, and hospital costs were higher in children with neurologic complications compared with those without complications. Factors associated with lower odds of neurologic complications included: younger age (adjusted odds ratio [aOR]: 0.97; 95% confidence interval [CI]: 0.96-0.98), occurrence during delta variant predominant time period (aOR: 0.71; 95% CI: 0.57-0.87), presence of a nonneurologic complex chronic condition (aOR: 0.80; 95% CI: 0.69-0.94). The presence of a neurologic complex chronic condition was associated with higher odds of neurologic complication (aOR 4.14, 95% CI 3.48-4.92).
Conclusions: Neurologic complications are common in children hospitalized with COVID-19 and are associated with worse hospital outcomes. Our findings emphasize the importance of COVID-19 immunization in children, especially in high-risk populations, such as those with neurologic comorbidity.
Copyright © 2022 by the American Academy of Pediatrics.
Conflict of interest statement
Figures

References
-
- American Academy of Pediatrics . Children and COVID-19: state-level data report. Available at: https://www.aap.org/en/pages/2019-novel-coronavirus- covid-19-infections.... Accessed April 28, 2022
-
- Saravanos GL, King CL, Deng L, et al. . Respiratory syncytial virus-associated neurologic complications in children: a systematic review and aggregated case series. J Pediatr. 2021;239:39–49.e9 - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
