

Clinicopathological differences, risk factors and prognostic scores for western patients with intestinal and diffuse-type gastric cancer
- PMID: 35949214
- PMCID: PMC9244993
- DOI: 10.4251/wjgo.v14.i6.1162
Clinicopathological differences, risk factors and prognostic scores for western patients with intestinal and diffuse-type gastric cancer
Abstract
Background: In the molecular era, the Laurén system is still a cost-effective and widely implemented classification for gastric cancer (GC) and it has been recently associated with clinical, histological and molecular features of these tumors. Despite recent advances in the understanding of the molecular biology of GC, there is a need to develop new prognostic tools for patient stratification in clinical practice. Thus, the identification of easily available prognostic factors in patients with intestinal and diffuse-type tumors can significantly improve risk assessment and patient stratification in GC.
Aim: To identify clinicopathological differences, risk factors, and to develop cost-effective prognostic scores for patients with intestinal and diffuse-type GC.
Methods: Retrospective study of all patients undergoing surgery for GC at a tertiary referral center from 2001 to 2019. 286 cases met inclusion criteria (intestinal: 190, diffuse: 96). Clinical data and gross findings were collected. All specimens were reviewed by two independent pathologists and a detailed protocol for histologic evaluation was followed. Five tissue microarrays (TMAs) were constructed and sections of the TMA block were immunostained for HERCEPTEST, MSH2, MSH6, MLH1 and PMS2. Statistical analyses were performed and prognostic scores were developed based on hazard ratios.
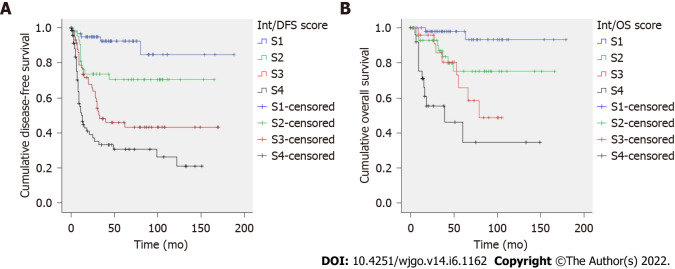
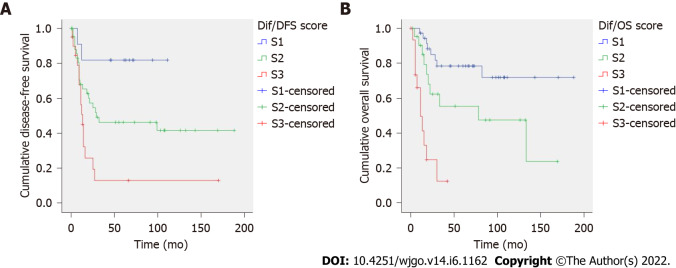
Results: Intestinal and diffuse-type GC showed different epidemiological, clinicopathological and prognostic features. Diffuse tumors were significantly associated with younger age, less symptomatology, flat morphology, deeper invasion, perineural infiltration, advanced stage at diagnosis, administration of adjuvant therapy and poorer prognosis. Intestinal lesions were fungoid or polypoid, showed necrosis, desmoplasia, microsatellite instability and HERCEPTEST positivity and were diagnosed at earlier stages. Tumor depth, desmoplasia, macroscopic type and lymph node involvement were independently related to the Laurén subtype. Furthermore, intestinal and diffuse GC were associated with different risk factors for progression and death. Vascular invasion, perineural infiltration and growth pattern were important prognostic factors in intestinal-type GC. On the contrary, tumor size and necrosis were significant prognosticators in diffuse-type GC. Our recurrence and cancer-specific death scores for patients with intestinal and diffuse-type GC showed an excellent patient stratification into three (diffuse GC) or four (intestinal) prognostic groups.
Conclusion: Our findings support that Laurén subtypes represent different clinicopathological and biological entities. The development of specific prognostic scores is a useful and cost-effective strategy to improve risk assessment in GC.
Keywords: Clinicopathological; Gastric cancer; Laurén; Molecular; Prognosis; Score.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: We have no financial relationships to disclose.
Figures
Similar articles
-
Proposal for a clinicopathological prognostic score for resected gastric cancer patients.Saudi J Gastroenterol. 2021 Jan-Feb;27(1):44-53. doi: 10.4103/sjg.SJG_208_20. Saudi J Gastroenterol. 2021. PMID: 33047677 Free PMC article.
-
Are Borrmann's Types of Advanced Gastric Cancer Distinct Clinicopathological and Molecular Entities? A Western Study.Cancers (Basel). 2021 Jun 21;13(12):3081. doi: 10.3390/cancers13123081. Cancers (Basel). 2021. PMID: 34205546 Free PMC article.
-
Development of a simplified tumor-lymph node ratio classification system for patients with resected gastric cancer: A western study.Ann Diagn Pathol. 2021 Feb;50:151677. doi: 10.1016/j.anndiagpath.2020.151677. Epub 2020 Dec 7. Ann Diagn Pathol. 2021. PMID: 33310591
-
Is there still a place for conventional histopathology in the age of molecular medicine? Laurén classification, inflammatory infiltration and other current topics in gastric cancer diagnosis and prognosis.Histol Histopathol. 2021 Jun;36(6):587-613. doi: 10.14670/HH-18-309. Epub 2021 Feb 10. Histol Histopathol. 2021. PMID: 33565601 Review.
-
The dawn of precision medicine in diffuse-type gastric cancer.Ther Adv Med Oncol. 2022 Mar 8;14:17588359221083049. doi: 10.1177/17588359221083049. eCollection 2022. Ther Adv Med Oncol. 2022. PMID: 35281349 Free PMC article. Review.
Cited by
-
Prognostic Significance of Lymph Node Ratio (LNR) in Gastric Cancer in Predicting Postoperative Complications and Survival: A Single-Center Study.Cancers (Basel). 2025 Feb 22;17(5):743. doi: 10.3390/cancers17050743. Cancers (Basel). 2025. PMID: 40075592 Free PMC article.
-
Involvement of Hormone Receptors, Membrane Receptors and Signaling Pathways in European Gastric Cancers Regarding Subtypes and Epigenetic Alterations: A Pilot Study.Biomedicines. 2025 Jul 24;13(8):1815. doi: 10.3390/biomedicines13081815. Biomedicines. 2025. PMID: 40868070 Free PMC article.
-
Liquid biopsy for gastric cancer: Techniques, applications, and future directions.World J Gastroenterol. 2024 Mar 28;30(12):1680-1705. doi: 10.3748/wjg.v30.i12.1680. World J Gastroenterol. 2024. PMID: 38617733 Free PMC article. Review.
-
Precancerous pathways to gastric cancer: a review of experimental animal models recapitulating the correa cascade.Front Cell Dev Biol. 2025 Jul 2;13:1620756. doi: 10.3389/fcell.2025.1620756. eCollection 2025. Front Cell Dev Biol. 2025. PMID: 40673273 Free PMC article. Review.
-
Diffuse Gastric Cancer: A Comprehensive Review of Molecular Features and Emerging Therapeutics.Target Oncol. 2024 Nov;19(6):845-865. doi: 10.1007/s11523-024-01097-2. Epub 2024 Sep 13. Target Oncol. 2024. PMID: 39271577 Free PMC article. Review.
References
-
- Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer. 2011;14:101–112. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
