

"Sitting-up vertigo as an expression of posterior semicircular canal heavy cupula and posterior semicircular canal short arm canalolithiasis"
- PMID: 35949549
- PMCID: PMC9349016
- DOI: 10.1016/j.joto.2022.02.001
"Sitting-up vertigo as an expression of posterior semicircular canal heavy cupula and posterior semicircular canal short arm canalolithiasis"
Abstract
Background: Vestibular symptoms on sitting-up are frequent on patients seen by vestibular specialists. Recently, a benign paroxysmal positional vertigo (BPPV) variant which elicits vestibular symptoms with oculomotor evidence of posterior semicircular canal (P-SCC) cupula stimulation on sitting-up was described and named sitting-up vertigo BPPV. A periampullar restricted P-SCC canalolithiasis was proposed as a causal mechanism.
Objective: To describe new mechanisms of action for the sitting-up vertigo BPPV variant.
Methods: Eighteen patients with sitting-up vertigo BPPV were examined with a pre-established set of positional maneuvers and follow-up until they resolved their symptoms and clinical findings.
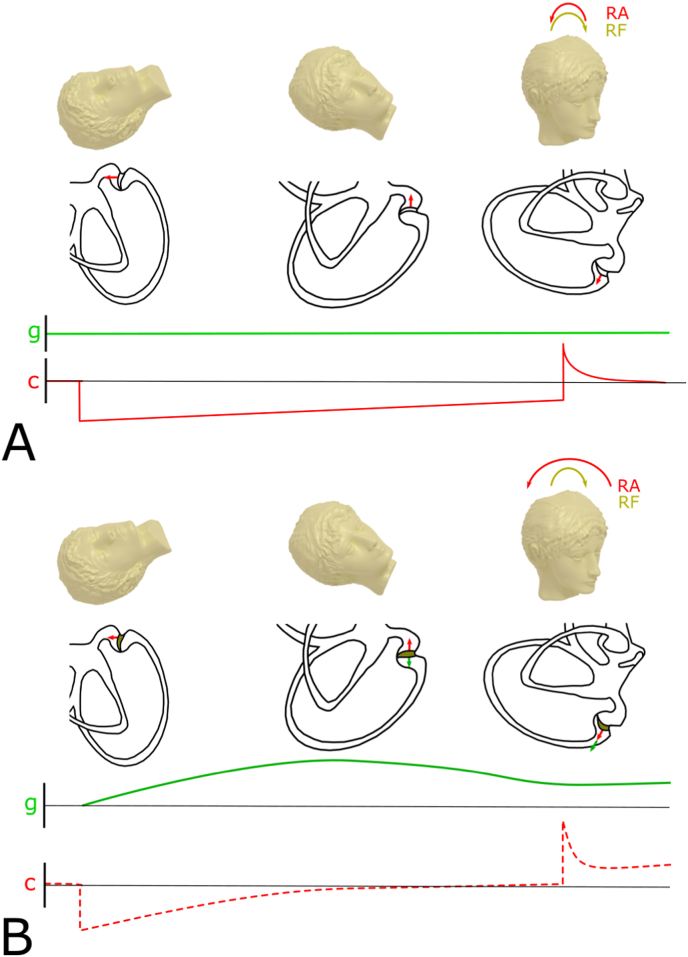
Results: All patients showed up-beating torsional nystagmus (UBTN) and vestibular symptoms on coming up from either Dix-Hallpike (DHM) or straight head-hanging maneuver. Sixteen out of 18 patients presented a sustained UBTN with an ipsitorsional component to the tested side on half-Hallpike maneuver (HH). A slower persistent contratorsional down-beating nystagmus was found in eleven out 18 patients tested on nose down position (ND).
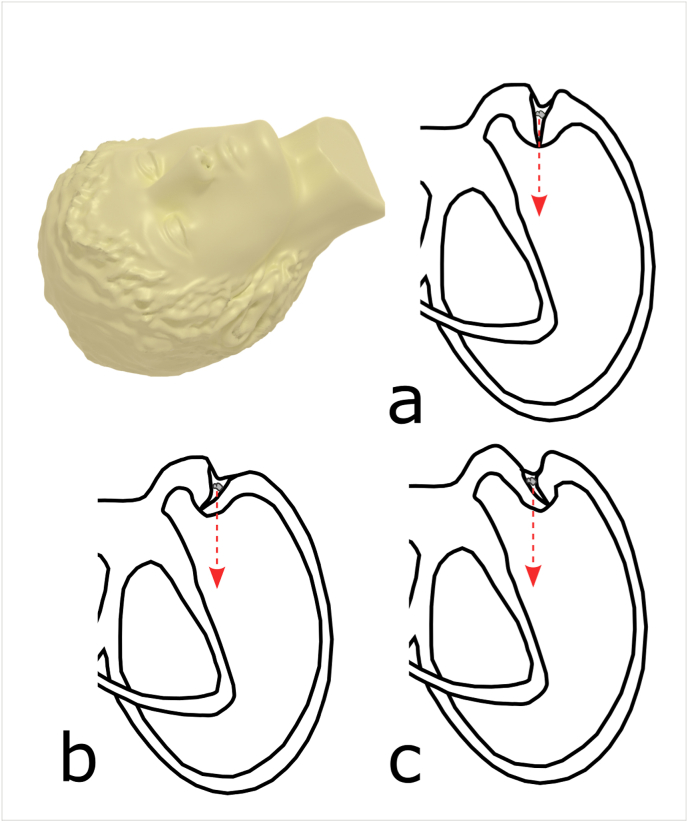
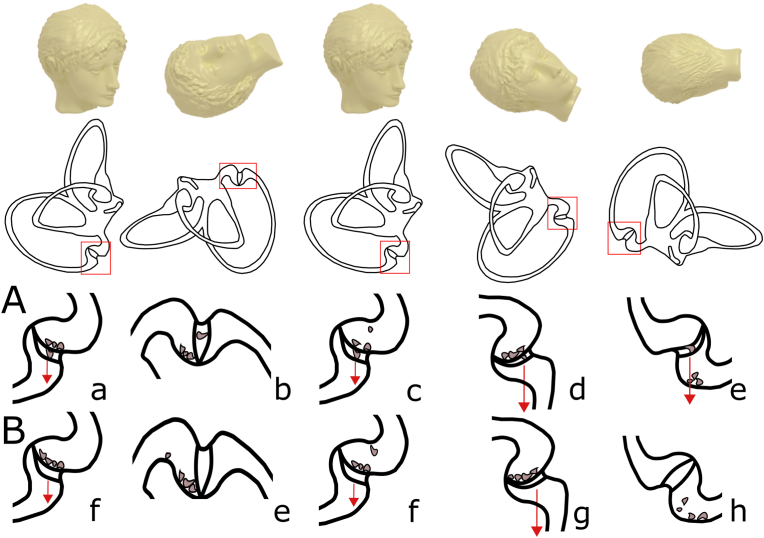
Conclusions: Persistent direction changing positional nystagmus on HH and ND positions indicative of P-SCC heavy cupula was found in 11 patients. A sustained UBTN on HH with the absence of findings on ND, which is suggestive of the presence of P-SCC short arm canalolithiasis, was found on 5 patients. All patients were treated with canalith repositioning maneuvers without success, but they resolved their findings by means of Brandt-Daroff exercises. We propose P-SCC heavy cupula and P-SCC short arm canalolithiasis as two new putative mechanisms for the sitting-up vertigo BPPV variant.
Keywords: BPPV; BPPV, benign paroxysmal positional vertigo; Benign paroxysmal positional vertigo; CRM, canalith repositioning maneuvers; DBTN, down-beating torsional nystagmus; DHM, Dix-Hallpike maneuver; HH, half-Hallpike maneuver; HYT, head yaw test; Heavy cupula; ND, nose down position; Residual dizziness; SCC, semicircular canal; SHH, straight head hanging; Short arm canalolithiasis; Sitting up vertigo; Subjective BPPV; UBTN, up-beating torsional nystagmus; Vertigo.
© 2022 PLA General Hospital Department of Otolaryngology Head and Neck Surgery. Production and hosting by Elsevier (Singapore) Pte Ltd.
Figures
Similar articles
-
Sitting Up Vertigo. Proposed Variant of Posterior Canal Benign Paroxysmal Positional Vertigo.Otol Neurotol. 2019 Apr;40(4):497-503. doi: 10.1097/MAO.0000000000002157. Otol Neurotol. 2019. PMID: 30870365
-
Benign paroxysmal positional vertigo.Auris Nasus Larynx. 2022 Oct;49(5):737-747. doi: 10.1016/j.anl.2022.03.012. Epub 2022 Apr 3. Auris Nasus Larynx. 2022. PMID: 35387740 Review.
-
Retrospective analysis of nystagmus characteristics and clinical applications of positional testing in patients with cupulolithiasis of the posterior semicircular canal in benign paroxysmal positional vertigo.Front Neurol. 2024 Jul 10;15:1413929. doi: 10.3389/fneur.2024.1413929. eCollection 2024. Front Neurol. 2024. PMID: 39050123 Free PMC article.
-
[Management of bilateral benign paroxysmal positional vertigo with Dix-Hallpike test].Zhonghua Nei Ke Za Zhi. 2014 Oct;53(10):764-7. Zhonghua Nei Ke Za Zhi. 2014. PMID: 25567145 Chinese.
-
Classification, diagnostic criteria and management of benign paroxysmal positional vertigo.Auris Nasus Larynx. 2017 Feb;44(1):1-6. doi: 10.1016/j.anl.2016.03.013. Epub 2016 May 9. Auris Nasus Larynx. 2017. PMID: 27174206 Review.
Cited by
-
Atypical Benign Paroxysmal Positional Vertigo: Concomitant Cupulolithiasis and Short-Arm Canalolithiasis Involving the Posterior Canal?J Clin Neurol. 2024 May;20(3):336-338. doi: 10.3988/jcn.2023.0445. J Clin Neurol. 2024. PMID: 38713078 Free PMC article. No abstract available.
-
Resolution of atypical posterior semicircular canal BPPV: evidence for putative short-arm location.BMJ Case Rep. 2023 May 29;16(5):e254579. doi: 10.1136/bcr-2023-254579. BMJ Case Rep. 2023. PMID: 37247949 Free PMC article.
-
Subjective BPPV revisited: identification of positional nystagmus with a new maneuver.J Neurol. 2024 Jul;271(7):4640-4643. doi: 10.1007/s00415-024-12347-8. Epub 2024 Apr 2. J Neurol. 2024. PMID: 38564054 No abstract available.
-
Atypical Bilateral Posterior Semicircular Canalolithiasis - A Case Series.Ann Indian Acad Neurol. 2024 Nov 1;27(6):720-723. doi: 10.4103/aian.aian_387_24. Epub 2024 Aug 1. Ann Indian Acad Neurol. 2024. PMID: 39083400 Free PMC article.
-
Atypical PC-BPPV - Cupulolithiasis and Short-Arm Canalithiasis: A Retrospective Observational Study.J Neurol Phys Ther. 2025 Jan 1;49(1):51-61. doi: 10.1097/NPT.0000000000000494. Epub 2024 Oct 16. J Neurol Phys Ther. 2025. PMID: 39656163 Free PMC article.
References
-
- Asprella Libonati G. Gravity sensitive cupula of posterior semicircular canal. Ann. N. Y. Acad. Sci. 2011;1233:188–199.
-
- Baloh R., Honrubia V., Kerber K.A. fourth ed. Oxford University Press; 2010. Baloh and Honrubia's Clinical Neurophysiology of the Vestibular System.
LinkOut - more resources
Full Text Sources
Research Materials
