

Treatment outcomes and relative dose intensity of chemotherapy in patients with advanced Hodgkin lymphoma
- PMID: 35949614
- PMCID: PMC9353858
- DOI: 10.3892/ol.2022.13440
Treatment outcomes and relative dose intensity of chemotherapy in patients with advanced Hodgkin lymphoma
Abstract
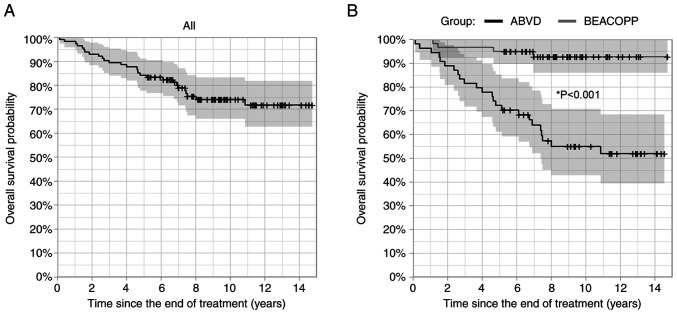
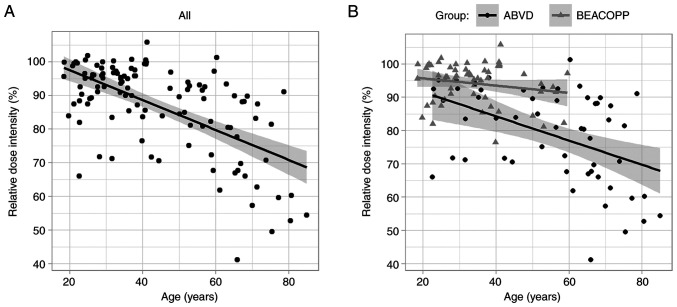
The present retrospective study was undertaken to investigate the association of relative dose intensity (RDI) with the outcome of patients with advanced stage Hodgkin lymphoma (HL) receiving ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) and escalated BEACOPP regimens (bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, prednisone). A total of 114 patients with HL treated between 2004 and 2013 were enrolled for evaluation. The association of variables with overall survival (OS) and progression-free survival (PFS) was analysed using univariate and multivariate Cox proportional hazards models. The median age of patients was 39 years, and the majority were male and had stage IV disease. A total of 54 patients received ABVD and 60 received BEACOPP chemotherapy with 24 and four deaths, respectively. Patients in the BEACOPP group were significantly younger with lower Charlson comorbidity index (CCI) and better performance status in comparison with the ABVD group, making the comparison of groups not possible. In the ABVD group, RDI was not significantly associated with OS (P=0.590) or PFS (P=0.354) in a multivariate model where age was controlled. The low number of events prevented this analysis in the BEACOPP group. The age of patients was strongly associated with both OS and PFS; all statistically significant predictors for OS and PFS from univariate analyses (chemotherapy regimen, CCI, RDI, performance status) lost their effect in multivariate analyses where age was controlled. Based on these observations, it was concluded that RDI was not associated with OS or PFS after age is controlled, neither in all patients combined nor in the ABVD group.
Keywords: Hodgkin lymphoma; chemotherapy; outcome; primary treatment; relative dose intensity.
Copyright: © Rožman et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Long-Term Results of the HD2000 Trial Comparing ABVD Versus BEACOPP Versus COPP-EBV-CAD in Untreated Patients With Advanced Hodgkin Lymphoma: A Study by Fondazione Italiana Linfomi.J Clin Oncol. 2016 Apr 10;34(11):1175-81. doi: 10.1200/JCO.2015.62.4817. Epub 2015 Dec 28. J Clin Oncol. 2016. PMID: 26712220 Clinical Trial.
-
Intensified treatment of patients with early stage, unfavourable Hodgkin lymphoma: long-term follow-up of a randomised, international phase 3 trial of the German Hodgkin Study Group (GHSG HD14).Lancet Haematol. 2021 Apr;8(4):e278-e288. doi: 10.1016/S2352-3026(21)00029-6. Lancet Haematol. 2021. PMID: 33770483 Clinical Trial.
-
Autotransplant for Hodgkin lymphoma after failure of upfront BEACOPP escalated (bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine and prednisone).Leuk Lymphoma. 2013 Jan;54(1):36-40. doi: 10.3109/10428194.2012.702903. Epub 2012 Jul 9. Leuk Lymphoma. 2013. PMID: 22702653
-
Long-term overall survival and toxicities of ABVD vs BEACOPP in advanced Hodgkin lymphoma: A pooled analysis of four randomized trials.Cancer Med. 2020 Sep;9(18):6565-6575. doi: 10.1002/cam4.3298. Epub 2020 Jul 25. Cancer Med. 2020. PMID: 32710498 Free PMC article. Review.
-
Comparison of the efficiency of ABVD versus BEACOPP for Hodgkin lymphoma treatment: a meta-analysis.Int J Hematol. 2016 Oct;104(4):413-9. doi: 10.1007/s12185-016-2080-5. Epub 2016 Aug 16. Int J Hematol. 2016. PMID: 27531149 Review.
Cited by
-
Treatment of older patients with Hodgkin lymphoma.Blood Res. 2025 Jun 12;60(1):35. doi: 10.1007/s44313-025-00084-4. Blood Res. 2025. PMID: 40504313 Free PMC article. Review.
References
-
- Howlader N, Noone AM, Krapcho M, Miller D, Brest A, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, et al. National Cancer Institute; Bethesda, MD: 2020. SEER cancer statistics review, 1975–2017, https://seer.cancer.gov/csr/1975_2017/ , based on November 2019 SEER data submission, posted to the SEER web site.
-
- Cheson BD, Fisher RI, Barrington SF, Cavalli F, Schwartz LH, Zucca E, Lister TA, Alliance, Australasian Leukaemia and Lymphoma Group and Eastern Cooperative Oncology Group et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J Clin Oncol. 2014;32:3059–3068. doi: 10.1200/JCO.2013.54.8800. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources