

Open-chest Pulsed Electric Field Ablation of Cardiac Ganglionated Plexi in Acute Canine Models
- PMID: 35949650
- PMCID: PMC9359425
- DOI: 10.19102/icrm.2022.130704
Open-chest Pulsed Electric Field Ablation of Cardiac Ganglionated Plexi in Acute Canine Models
Abstract
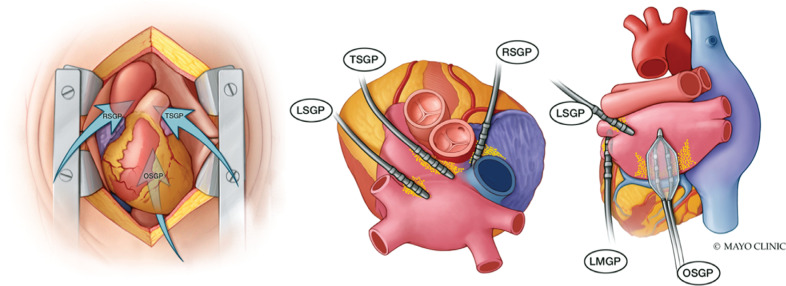
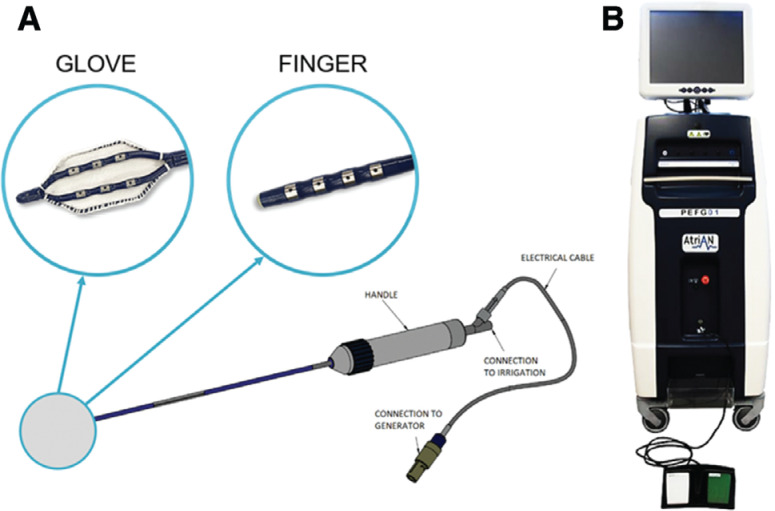
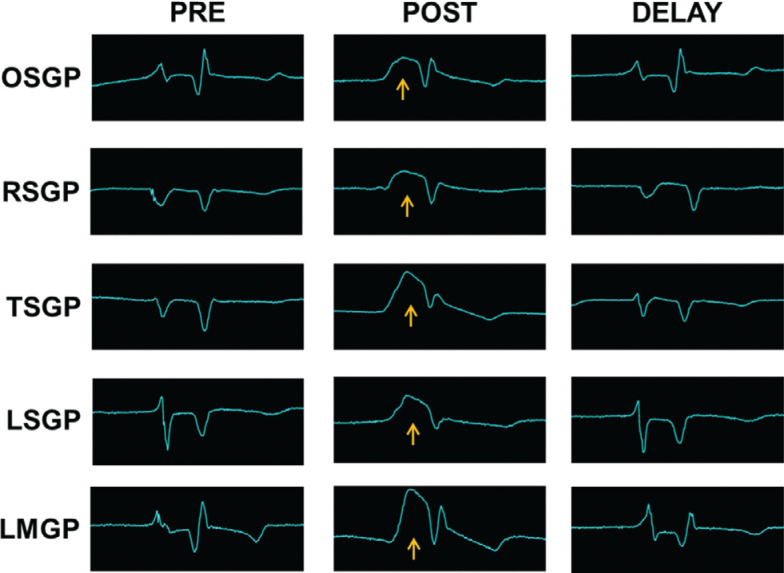
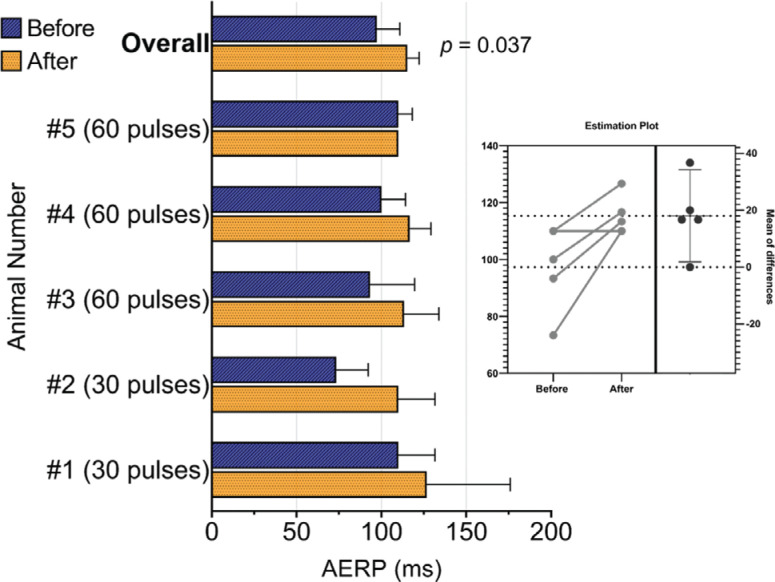
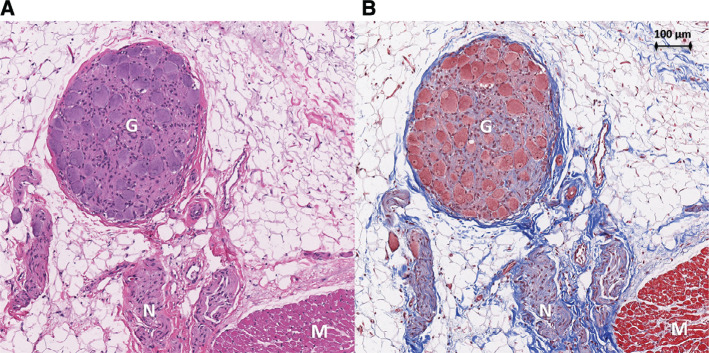
This study aimed to evaluate the safety and acute effect on markers of cardiac autonomic tone following pulsed electric fields (PEFs) delivered to epicardial ganglionated plexi (GP) during a cardiac surgical procedure. Ablation of GP as a treatment for atrial fibrillation (AF) has shown promise, but thermal ablation energy sources are limited by the risk of inadvertent collateral tissue injury. In acute canine experiments, median sternotomy was performed to facilitate the identification of 5 epicardial GP regions using an anatomy-guided approach. Each site was targeted with saline-irrigated PEF (1000 V, 100 μs, 10 electrocardiogram [ECG]-synchronized pulse sequences). Atrial effective refractory period (AERP) and local electrogram (EGM) amplitude were measured before and after each treatment. Histology was performed on samples from treatment-adjacent structures. In 5 animals, 30 (n = 2) and 60 (n = 3) pulses were successfully delivered to each of the 5 target sites. There was no difference in local atrial EGM amplitude before and after PEF application at each site (1.83 ± 0.41 vs. 1.92 ± 0.53 mV, P = .72). The mean AERP increased from 97 ± 15 ms at baseline to 115 ± 7 ms following treatment at all sites (18.6% increase; 95% confidence interval, 1.9-35.2; P = .037). There were no sustained ventricular arrhythmias or acute evidence of ischemia following delivery. Histology showed complete preservation of adjacent atrial myocardium, phrenic nerves, pericardium, and esophagus. Use of PEF to target regions rich in cardiac GP in open-chest canine experiments was feasible and effective at acutely altering markers of cardiac autonomic tone.
Keywords: Ganglionated plexi; atrial fibrillation; cardiac denervation; electroporation; pulsed electric fields.
Copyright: © 2022 Innovations in Cardiac Rhythm Management.
Conflict of interest statement
Mayo Clinic has pursued protection of intellectual property including in the form of patents and patent applications, naming Dr. Asirvatham as inventor, related to the information disclosed herein, and licensed to AtriAN Medical Ltd. Mr. Reilly, Dr. O’Brien, and Mr. Coffey are employed by AtriAN Medical Ltd., which provided funding for this study and supplied the preclinical generator and catheters used. The other authors report no conflicts of interest for the published content. This study was reviewed by the Mayo Clinic Conflict of Interest Review Board and was conducted in compliance with Mayo Clinic Conflict of Interest policies. Funding for this study was provided by AtriAN Medical Ltd.
Figures
Similar articles
-
Targeted epicardial pulsed field ablation of atrial ganglionated plexi: Electrophysiological and histologic analysis in pigs.Heart Rhythm. 2025 Jun 17:S1547-5271(25)02562-7. doi: 10.1016/j.hrthm.2025.06.016. Online ahead of print. Heart Rhythm. 2025. PMID: 40553918
-
Novel Percutaneous Epicardial Autonomic Modulation in the Canine for Atrial Fibrillation: Results of an Efficacy and Safety Study.Pacing Clin Electrophysiol. 2016 May;39(5):407-17. doi: 10.1111/pace.12824. Epub 2016 Mar 9. Pacing Clin Electrophysiol. 2016. PMID: 26854009 Free PMC article.
-
Pulsed Electric Field Ablation of Epicardial Autonomic Ganglia: Computer Analysis of Monopolar Electric Field across the Tissues Involved.Bioengineering (Basel). 2022 Nov 27;9(12):731. doi: 10.3390/bioengineering9120731. Bioengineering (Basel). 2022. PMID: 36550937 Free PMC article.
-
Ganglionated plexi as neuromodulation targets for atrial fibrillation.J Cardiovasc Electrophysiol. 2017 Dec;28(12):1485-1491. doi: 10.1111/jce.13319. Epub 2017 Sep 8. J Cardiovasc Electrophysiol. 2017. PMID: 28833764 Free PMC article. Review.
-
Is the Atrial Neural Plexis a Therapeutic Target in Atrial Fibrillation?Methodist Debakey Cardiovasc J. 2015 Apr-Jun;11(2):82-6. doi: 10.14797/mdcj-11-2-82. Methodist Debakey Cardiovasc J. 2015. PMID: 26306124 Free PMC article. Review.
Cited by
-
Development of neuromodulation for atrial fibrillation: a narrative review.J Thorac Dis. 2024 May 31;16(5):3472-3483. doi: 10.21037/jtd-23-1981. Epub 2024 May 20. J Thorac Dis. 2024. PMID: 38883655 Free PMC article. Review.
-
Cardiac Radiofrequency Ablation Exacerbates Myocardial Injury through Pro-Inflammatory Response and Pro-Oxidative Stress in Elderly Patients with Persistent Atrial Fibrillation.Curr Vasc Pharmacol. 2024;22(2):137-152. doi: 10.2174/0115701611257644231215071611. Curr Vasc Pharmacol. 2024. PMID: 38213173
-
Epicardial Pulsed Field Ablation of Ganglionated Plexi: Computational and Pre-Clinical Evaluation of a Bipolar Sub-Xiphoid Catheter for the Treatment of Atrial Fibrillation.Bioengineering (Basel). 2023 Dec 24;11(1):18. doi: 10.3390/bioengineering11010018. Bioengineering (Basel). 2023. PMID: 38247895 Free PMC article.
-
Letter from the Editor in Chief.J Innov Card Rhythm Manag. 2022 Jul 15;13(7):A7. doi: 10.19102/icrm.2022.130707. eCollection 2022 Jul. J Innov Card Rhythm Manag. 2022. PMID: 35949647 Free PMC article. No abstract available.
-
Targeted ablation of epicardial ganglionated plexi during cardiac surgery with pulsed field electroporation (NEURAL AF).J Interv Card Electrophysiol. 2025 Mar;68(2):467-474. doi: 10.1007/s10840-023-01615-8. Epub 2023 Aug 10. J Interv Card Electrophysiol. 2025. PMID: 37561246 Free PMC article. Clinical Trial.
References
-
- Mathew JP, Fontes ML, Tudor IC, et al. A multicenter risk index for atrial fibrillation after cardiac surgery. J Am Med Assoc. 2004;291(14):1720–1729. [CrossRef] [PubMed] - DOI - PubMed
-
- Melduni RM, Schaff HV, Bailey KR, et al. Implications of new-onset atrial fibrillation after cardiac surgery on long-term prognosis: a community-based study. Am Heart J. 2015;170(4):659–668. [CrossRef] [PubMed] - DOI - PubMed
-
- Welch TD, Coylewright M, Powell BD, et al. Symptomatic pulmonary hypertension with giant left atrial v waves after surgical maze procedures: evaluation by comprehensive hemodynamic catheterization. Heart Rhythm. 2013;10(12):1839–1842. [CrossRef] [PubMed] - DOI - PubMed
-
- Ishii Y, Gleva MJ, Gamache MC, et al. Atrial tachyarrhythmias after the maze procedure: incidence and prognosis. Circulation. 2004;110(11 Suppl 1):II164–II168. [CrossRef] [PubMed] - DOI - PubMed
-
- Fenstad ER, Hardegree EL, Le RJ, et al. Hemodynamic changes after surgical MAZE: pulmonary hypertension secondary to stiff left atrial syndrome? J Heart Lung Transpl. 2013;32(4):S62–S62. doi: 10.1016/j.healun.2013.01.968. - DOI
LinkOut - more resources
Full Text Sources