

Managements of osteoporotic vertebral compression fractures: A narrative review
- PMID: 35949707
- PMCID: PMC9244957
- DOI: 10.5312/wjo.v13.i6.564
Managements of osteoporotic vertebral compression fractures: A narrative review
Abstract
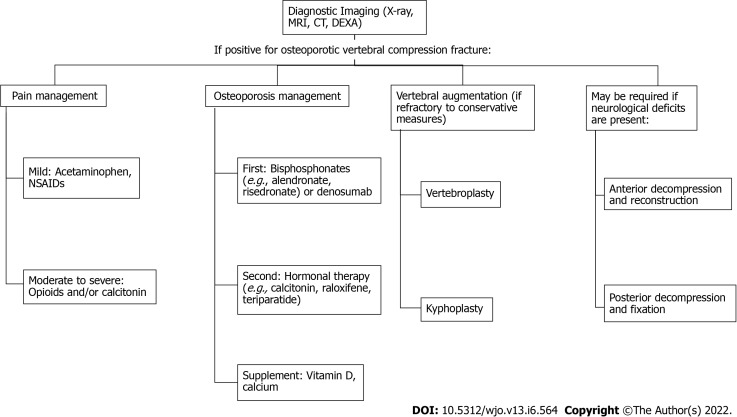
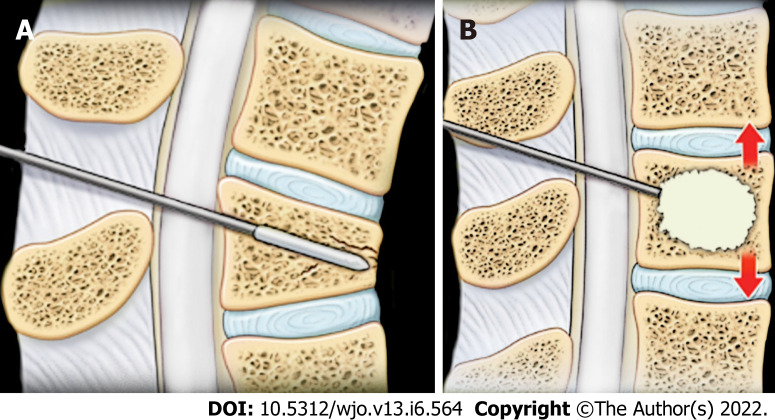
Osteoporotic vertebral compression fractures (OVCFs) are the most common fragility fracture and significantly influence the quality of life in the elderly. Currently, the literature lacks a comprehensive narrative review of the management of OVCFs. The purpose of this study is to review background information, diagnosis, and surgical and non-surgical management of the OVCFs. A comprehensive search of PubMed and Google Scholar for articles in the English language between 1980 and 2021 was performed. Combinations of the following terms were used: compression fractures, vertebral compression fractures, osteoporosis, osteoporotic compression fractures, vertebroplasty, kyphoplasty, bisphosphonates, calcitonin, and osteoporosis treatments. Additional articles were also included by examining the reference list of articles found in the search. OVCFs, especially those that occur over long periods, can be asymptomatic. Symptoms of acute OVCFs include pain localized to the mid-line spine, a loss in height, and decreased mobility. The primary treatment regimens are pain control, medication management, vertebral augmentation, and anterior or posterior decompression and reconstructions. Pain control can be achieved with acetaminophen or nonsteroidal anti-inflammatory drugs for mild pain or opioids and/or calcitonin for moderate to severe pain. Bisphosphonates and denosumab are the first-line treatments for osteoporosis. Vertebroplasty and kyphoplasty are reserved for patients who have not found symptomatic relief through conservative methods and are effective in achieving pain relief. Vertebroplasty is less technical and cheaper than kyphoplasty but could have more complications. Calcium and vitamin D supplementation can have a protective and therapeutic effect. Management of OVCFs must be combined with multiple approaches. Appropriate exercises and activity modification are important in fracture prevention. Medication with different mechanisms of action is a critical long-term causal treatment strategy. The minimally invasive surgical interventions such as vertebroplasty and kyphoplasty are reserved for patients not responsive to conservative therapy and are recognized as efficient stopgap treatment methods. Posterior decompression and fixation or Anterior decompression and reconstruction may be required if neurological deficits are present. The detailed pathogenesis and related targeted treatment options still need to be developed for better clinical outcomes.
Keywords: Fragility fractures; Kyphoplasty; Osteoporosis; Osteoporotic vertebral compression fractures; Vertebral body; Vertebroplasty.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All authors declare that they have no conflicts of interest in creating and publishing this manuscript and received no funding to assist in its completion.
Figures
References
-
- Riggs BL, Melton LJ 3rd. The worldwide problem of osteoporosis: insights afforded by epidemiology. Bone. 1995;17:505S–511S. - PubMed
-
- Marwick C. Consensus Panel Considers Osteoporosis. JAMA. 2000;283:2093–2095. - PubMed
-
- Oleksik A, Lips P, Dawson A, Minshall ME, Shen W, Cooper C, Kanis J. Health-related quality of life in postmenopausal women with low BMD with or without prevalent vertebral fractures. J Bone Miner Res. 2000;15:1384–1392. - PubMed
-
- Oleksik AM, Ewing S, Shen W, van Schoor NM, Lips P. Impact of incident vertebral fractures on health related quality of life (HRQOL) in postmenopausal women with prevalent vertebral fractures. Osteoporos Int. 2005;16:861–870. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
