

Effects of Renin-Angiotensin-Aldosterone System Inhibition on Left Ventricular Hypertrophy, Diastolic Function, and Functional Status in Patients With Hypertrophic Cardiomyopathy: A Systematic Review
- PMID: 35949750
- PMCID: PMC9356743
- DOI: 10.7759/cureus.26642
Effects of Renin-Angiotensin-Aldosterone System Inhibition on Left Ventricular Hypertrophy, Diastolic Function, and Functional Status in Patients With Hypertrophic Cardiomyopathy: A Systematic Review
Abstract
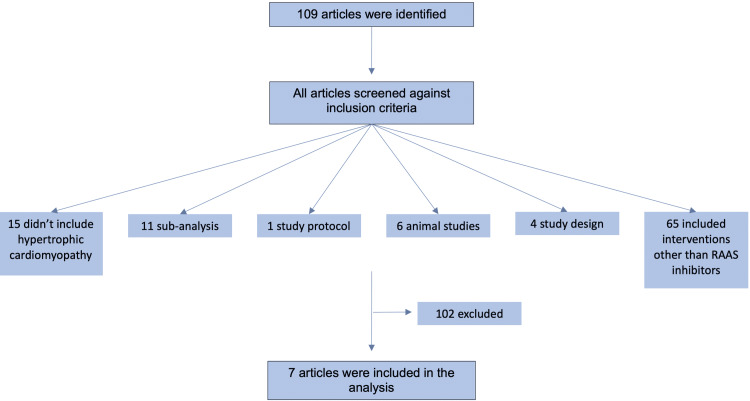
The renin-angiotensin-aldosterone system (RAAS) plays a vital role in cardiovascular homeostasis by regulating blood pressure, salt, and water balance. The kidneys produce renin which converts angiotensinogen to angiotensin-1 (AT-I) and angiotensin-converting enzyme (ACE) to angiotensin-II (AT-II). AT-II binds to receptors in the adrenal cortex to release aldosterone. AT-II and aldosterone promote water and salt retention, vascular tone, and myocardial contractility. These physiological changes raise blood pressure and circulation. Reduced renal perfusion pressure sensed by baroreceptors and the sympathetic nervous system's β-adrenergic receptors trigger renin release and RAAS activation. RAAS restores hemodynamic stability in pathological states associated with low perfusion. This adaptive response is important for restoring perfusion and hemodynamic stability, but prolonged RAAS activation has deleterious effects on the cardiovascular system. Long-term mineralocorticoid exposure has been linked to left ventricular hypertrophy (LVH) and remodeling. AT-II activates fibroblasts and cardiac myocytes to promote cardiac remodeling. Blocking RAAS can eliminate the long-term negative effects of RAAS activation. Direct renin inhibitors, ACE inhibitors, angiotensin receptor blockers, and aldosterone antagonists are RAAS blockers. RAAS blockade improves mortality and hospitalization in systolic heart failure and acute myocardial infarction. RAAS blockade has not demonstrated the same benefits in other cardiac populations, such as those with preserved ejection fraction. Hypertrophic cardiomyopathy (HCM) causes LVH and asymmetric septal hypertrophy. When the outflow tract gradient exceeds 30 mmHg and is associated with septal hypertrophy, it is known as obstructive HCM. Dyspnea on exertion, syncope, and exertional angina are symptoms of HCM. RAAS activation worsens LVH by increasing blood pressure and by directly affecting cardiac myocytes with AT-II and aldosterone. RAAS blockade reverses myocardial fibrosis and slows HCM progression in animal models. We performed a meta-analysis of randomized clinical trials to further investigate the potential benefit of RAAS blockade in HCM patients. Although our findings included significant results for some of the RAAS blockade agents, these findings were not consistent throughout all the studies. Mavacamten, one of the newest treatments, has shown promising outcomes.
Keywords: functional status; left ventricular diastolic dysfunction; left ventricular hypertrophy (lvh); raas inhibitors; systematic review.
Copyright © 2022, Akhtar et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Optimal antagonism of the Renin-Angiotensin-aldosterone system: do we need dual or triple therapy?Drugs. 2010 Jul 9;70(10):1215-30. doi: 10.2165/11537910-000000000-00000. Drugs. 2010. PMID: 20568830 Review.
-
Myocardial fibrosis in patients with symptomatic obstructive hypertrophic cardiomyopathy: correlation with echocardiographic measurements, sarcomeric genotypes, and pro-left ventricular hypertrophy polymorphisms involving the renin-angiotensin-aldosterone system.Cardiovasc Pathol. 2009 Sep-Oct;18(5):262-8. doi: 10.1016/j.carpath.2008.08.003. Epub 2008 Oct 2. Cardiovasc Pathol. 2009. PMID: 18835191
-
Exploring the implications of blocking renin-angiotensin-aldosterone system and fibroblast growth factor 23 in early left ventricular hypertrophy without chronic kidney disease.Front Endocrinol (Lausanne). 2023 Dec 19;14:1276664. doi: 10.3389/fendo.2023.1276664. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 38174329 Free PMC article.
-
Pathophysiologic role of the renin-angiotensin-aldosterone and sympathetic nervous systems in heart failure.Am J Health Syst Pharm. 2004 May 1;61 Suppl 2:S4-13. doi: 10.1093/ajhp/61.suppl_2.S4. Am J Health Syst Pharm. 2004. PMID: 15160833 Review.
-
Role of angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, and aldosterone antagonists in the prevention of atrial and ventricular arrhythmias.Pharmacotherapy. 2009 Jan;29(1):31-48. doi: 10.1592/phco.29.1.31. Pharmacotherapy. 2009. PMID: 19113795 Review.
Cited by
-
Progress in the treatment of diabetic cardiomyopathy, a systematic review.Pharmacol Res Perspect. 2024 Apr;12(2):e1177. doi: 10.1002/prp2.1177. Pharmacol Res Perspect. 2024. PMID: 38407563 Free PMC article.
-
Drugs for treating myocardial fibrosis.Front Pharmacol. 2023 Sep 12;14:1221881. doi: 10.3389/fphar.2023.1221881. eCollection 2023. Front Pharmacol. 2023. PMID: 37771726 Free PMC article. Review.
-
The Role of Signalling Pathways in Myocardial Fibrosis in Hypertrophic Cardiomyopathy.Rev Cardiovasc Med. 2025 Feb 21;26(2):27152. doi: 10.31083/RCM27152. eCollection 2025 Feb. Rev Cardiovasc Med. 2025. PMID: 40026508 Free PMC article. Review.
-
The Molecular Mechanism and Therapeutic Strategy of Cardiorenal Syndrome Type 3.Rev Cardiovasc Med. 2023 Feb 6;24(2):52. doi: 10.31083/j.rcm2402052. eCollection 2023 Feb. Rev Cardiovasc Med. 2023. PMID: 39077418 Free PMC article. Review.
-
Safety of esaxerenone (CS-3150) and its impacts on blood pressure and renal function: A systematic review and meta-analysis.Medicine (Baltimore). 2025 Aug 1;104(31):e43615. doi: 10.1097/MD.0000000000043615. Medicine (Baltimore). 2025. PMID: 40760566 Free PMC article.
References
-
- Cellular and intrarenal control of renin secretion. Skøtt O, Jensen BL. Clin Sci (Lond) 1993;84:1–10. - PubMed
-
- Aldosterone and left ventricular remodeling. Catena C, Colussi G, Brosolo G, Novello M, Sechi LA. Horm Metab Res. 2015;47:981–986. - PubMed
-
- Molecular characterization of angiotensin II--induced hypertrophy of cardiac myocytes and hyperplasia of cardiac fibroblasts. Critical role of the AT1 receptor subtype. Sadoshima J, Izumo S. Circ Res. 1993;73:413–423. - PubMed
-
- Inhibition of the renin angiotensin aldosterone system: focus on aliskiren. Rao MS. https://pubmed.ncbi.nlm.nih.gov/20653151/ J Assoc Physicians India. 2010;58:102–108. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous