

Modified endoscopic ultrasound-guided selective N-butyl-2-cyanoacrylate injections for gastric variceal hemorrhage in left-sided portal hypertension: A case report
- PMID: 35949826
- PMCID: PMC9254179
- DOI: 10.12998/wjcc.v10.i18.6254
Modified endoscopic ultrasound-guided selective N-butyl-2-cyanoacrylate injections for gastric variceal hemorrhage in left-sided portal hypertension: A case report
Abstract
Background: Left-sided portal hypertension (LSPH), also known as sinistral portal hypertension or regional portal hypertension, refers to extrahepatic portal hypertension caused by splenic vein obstruction or stenosis. N-butyl-2-cyanoacrylate (NBC) has been widely used in the endoscopic hemostasis of portal hypertension, but adverse events including renal or pulmonary thromboembolism, mucosal necrosis and gastrointestinal (GI) bleeding may occur after treatment. Herein, we report successfully managing gastric variceal (GV) hemorrhage secondary to LSPH using modified endoscopic ultrasound (EUS)-guided selective NBC injections.
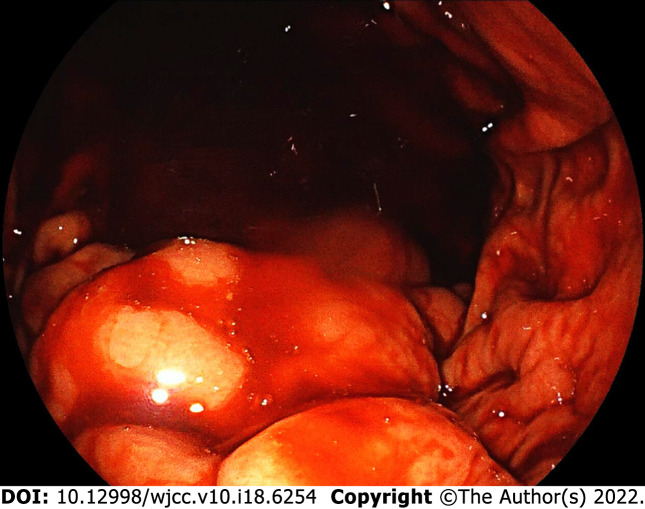
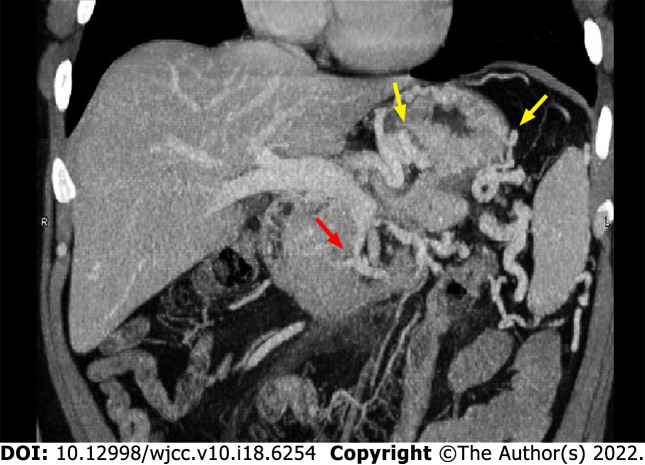
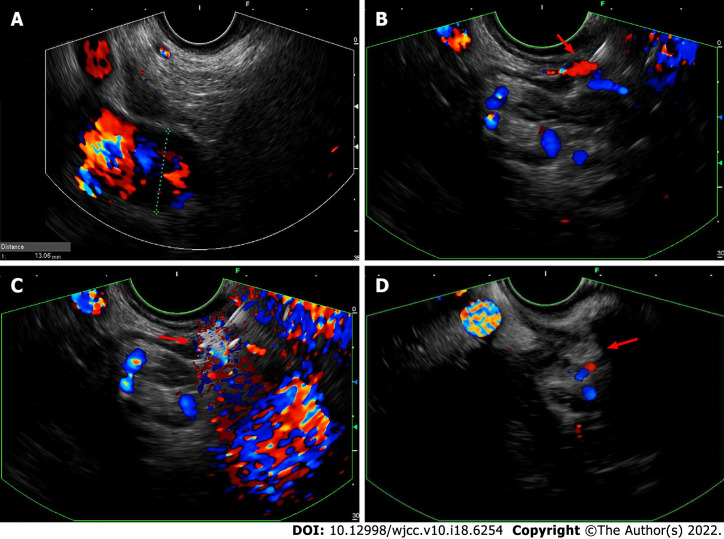
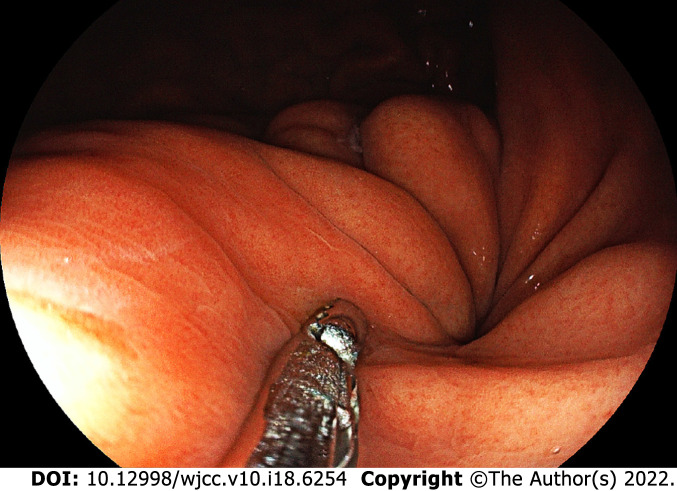
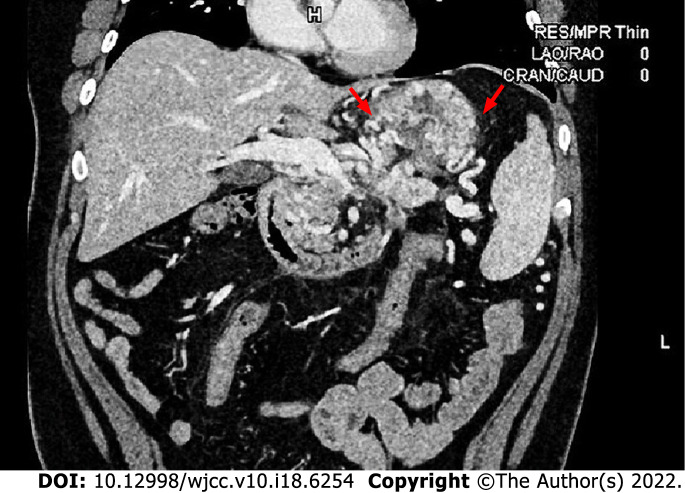
Case summary: A 35-year-old man was referred to our hospital due to an upper GI hemorrhage. Gastroscopy revealed GV hemorrhage and computed tomography venography (CTV) confirmed LSPH. The patient requested endoscopic procedures and rejected surgical therapies including splenectomy. EUS-guided selective NBC injections were performed and confluences of gastric varices were selected as the injection sites to reduce the injection dose. The "sandwich" method using undiluted NBC and hypertonic glucose was applied. No complications occurred. The patient was followed up regularly after discharge. Three months later, the follow-up gastroscopy revealed firm gastric submucosa with no sign of NBC expulsion and the follow-up CTV showed improvements in LSPH. No recurrent GI hemorrhage was reported during this follow-up period.
Conclusion: EUS-guided selective NBC injection may represent an effective and economical treatment for GV hemorrhage in patients with LSPH.
Keywords: Case report; Endoscopic ultrasound; Gastric varices; Left-sided portal hypertension; N-butyl-2-cyanoacrylate; Selective.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Safety and efficacy of modified endoscopic ultrasound-guided selective N-butyl-2-cyanoacrylate injections for gastric variceal hemorrhage in left-sided portal hypertension.World J Gastrointest Endosc. 2024 Jan 16;16(1):29-36. doi: 10.4253/wjge.v16.i1.29. World J Gastrointest Endosc. 2024. PMID: 38313456 Free PMC article.
-
EUS-guided fine needle injection is superior to direct endoscopic injection of 2-octyl cyanoacrylate for the treatment of gastric variceal bleeding.Surg Endosc. 2019 Jun;33(6):1837-1845. doi: 10.1007/s00464-018-6462-z. Epub 2018 Sep 26. Surg Endosc. 2019. PMID: 30259158
-
Gastric Varices in Cirrhosis versus Extrahepatic Portal Venous Obstruction and Response to Endoscopic N-Butyl-2-cyanoacrylate Injection.J Clin Exp Hepatol. 2013 Mar;3(1):19-23. doi: 10.1016/j.jceh.2013.01.002. Epub 2013 Jan 25. J Clin Exp Hepatol. 2013. PMID: 25755467 Free PMC article.
-
Utility of endoscopic ultrasound in patients with portal hypertension.World J Gastroenterol. 2014 Oct 21;20(39):14230-6. doi: 10.3748/wjg.v20.i39.14230. World J Gastroenterol. 2014. PMID: 25339809 Free PMC article. Review.
-
Left-sided portal hypertension caused by peripancreatic lymph node tuberculosis misdiagnosed as pancreatic cancer: a case report and literature review.BMC Gastroenterol. 2020 Aug 18;20(1):276. doi: 10.1186/s12876-020-01420-x. BMC Gastroenterol. 2020. PMID: 32811429 Free PMC article. Review.
Cited by
-
Endoscopic ultrasound-guided diagnosis and treatment of gastric varices.World J Gastrointest Endosc. 2022 Dec 16;14(12):748-758. doi: 10.4253/wjge.v14.i12.748. World J Gastrointest Endosc. 2022. PMID: 36567822 Free PMC article. Review.
-
Endoscopic Ultrasound in Pancreatology: Focus on Inflammatory Diseases and Interventions.Visc Med. 2023 Oct;39(5):131-139. doi: 10.1159/000533433. Epub 2023 Sep 5. Visc Med. 2023. PMID: 37899796 Free PMC article. Review.
-
Case report: Upper gastrointestinal bleeding associated with pancreatic segmental portal hypertension: six case reports and literature review.Front Med (Lausanne). 2025 Feb 19;12:1522413. doi: 10.3389/fmed.2025.1522413. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40046926 Free PMC article.
-
Safety and efficacy of modified endoscopic ultrasound-guided selective N-butyl-2-cyanoacrylate injections for gastric variceal hemorrhage in left-sided portal hypertension.World J Gastrointest Endosc. 2024 Jan 16;16(1):29-36. doi: 10.4253/wjge.v16.i1.29. World J Gastrointest Endosc. 2024. PMID: 38313456 Free PMC article.
-
Necessity and Reconstruction Methods of Splenic Vein After Resection of the Portomesenteric Junction During Resections for Pancreatic Cancer.Curr Oncol. 2025 May 30;32(6):316. doi: 10.3390/curroncol32060316. Curr Oncol. 2025. PMID: 40558259 Free PMC article. Review.
References
-
- Xie CL, Wu CQ, Chen Y, Chen TW, Xue HD, Jin ZY, Zhang XM. Sinistral Portal Hypertension in Acute Pancreatitis: A Magnetic Resonance Imaging Study. Pancreas. 2019;48:187–192. - PubMed
-
- Köklü S, Coban S, Yüksel O, Arhan M. Left-sided portal hypertension. Dig Dis Sci. 2007;52:1141–1149. - PubMed
-
- Cheng LF, Wang ZQ, Li CZ, Cai FC, Huang QY, Linghu EQ, Li W, Chai GJ, Sun GH, Mao YP, Wang YM, Li J, Gao P, Fan TY. Treatment of gastric varices by endoscopic sclerotherapy using butyl cyanoacrylate: 10 years' experience of 635 cases. Chin Med J (Engl) 2007;120:2081–2085. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
