

Insulinoma after sleeve gastrectomy: A case report
- PMID: 35949856
- PMCID: PMC9254200
- DOI: 10.12998/wjcc.v10.i18.6227
Insulinoma after sleeve gastrectomy: A case report
Abstract
Background: Laparoscopic sleeve gastrectomy (LSG) has been proposed as an effective and durable treatment for severe obesity and glucose metabolism disorders, and its prevalence has increased from 5% to 37% since 2008. One common complication after bariatric surgery is a postprandial hyperinsulinemic hypoglycemic state. While rare, insulinomas can cause this state, where symptoms are more common in the fasting state; thus, evaluation of insulin secretion is needed. Until now, there have been no reports of insulinoma after LSG.
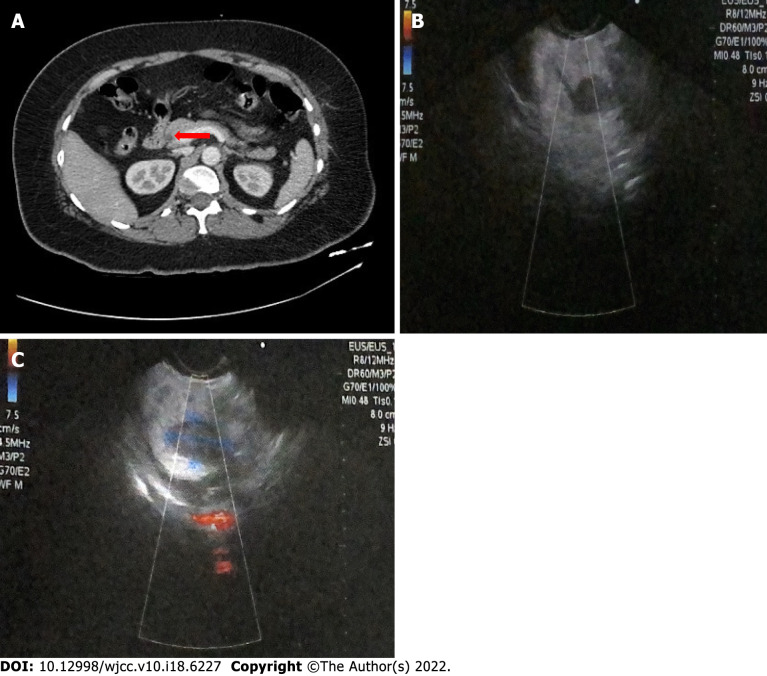
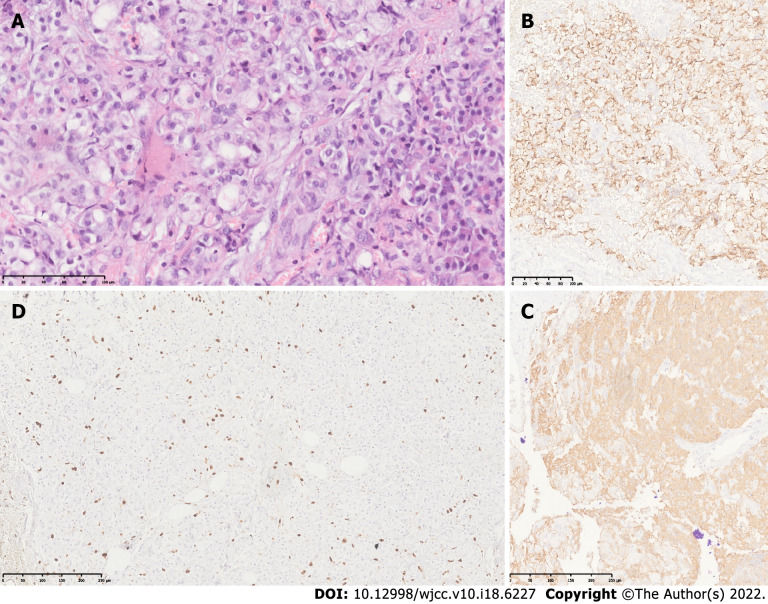
Case summary: We describe the case of a 43-year-old woman who was referred to the obesity clinic 2 years after LSG was performed. She had symptoms of hypoglycemia predominantly in the fasting state and documented hypoglycemia of less than 30 mg/dL, which are compatible with Whipple's triad. Initially, dumping syndrome was suspected, but after a second low fasting plasma glucose was documented, a 72-h fasting test was performed that tested positive. Computed tomography and endoscopic ultrasound were performed, identifying the presence of a homogeneous hypoechoic semioval tumoral lesion in the pancreas. The diagnosis was compatible with insulinoma. After laparoscopic enucleation of the insulinoma, the symptoms and hypoglycemia disappeared. The histopathological report described a well-differentiated grade 2 neuroendocrine tumor with positive chromogranin and synaptophysin and Ki67 immunopositivity in 4% of the neoplastic cells.
Conclusion: Insulinoma after LSG is a rare condition, and clinicians must be aware of it, especially if the patient has hypoglycemic symptoms during the fasting state.
Keywords: Bariatric surgery; Case report; Glucagon-like peptide 1 amide; Hypoglycemia; Insulinoma; Neuroendocrine tumors.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest to disclose.
Figures
Similar articles
-
A Five-Year Journey to Diagnosis: Resolving Persistent Hypoglycemia Through Successful Insulinoma Resection-A Case Report.Clin Case Rep. 2025 Mar 21;13(3):e70359. doi: 10.1002/ccr3.70359. eCollection 2025 Mar. Clin Case Rep. 2025. PMID: 40124204 Free PMC article.
-
Not Just an Accident: A Case of Insulinoma.Cureus. 2023 Nov 8;15(11):e48514. doi: 10.7759/cureus.48514. eCollection 2023 Nov. Cureus. 2023. PMID: 38074057 Free PMC article.
-
Insulinoma Unmasked Post Sleeve Gastrectomy With Incidental Renal Cell Carcinoma: A Rare Case.Cureus. 2024 May 15;16(5):e60395. doi: 10.7759/cureus.60395. eCollection 2024 May. Cureus. 2024. PMID: 38883112 Free PMC article.
-
Case presentation of 8-year follow up of recurrent malignant duodenal Insulinoma and lymph node metastases and literature review of malignant Insulinoma management.BMC Endocr Disord. 2022 Dec 9;22(1):310. doi: 10.1186/s12902-022-01219-9. BMC Endocr Disord. 2022. PMID: 36494838 Free PMC article. Review.
-
Sporadic insulinoma in a 10-year-old boy: a case report and literature review.JOP. 2014 Jan 10;15(1):53-7. doi: 10.6092/1590-8577/1925. JOP. 2014. PMID: 24413786 Review.
Cited by
-
Recurrent Hypoglycemia After Total Gastrectomy: A Case Report and Literature Analysis.Am J Case Rep. 2024 Jun 26;25:e943144. doi: 10.12659/AJCR.943144. Am J Case Rep. 2024. PMID: 38918938 Free PMC article. Review.
References
-
- Molina-Ayala M, Rodríguez-González A, Albarrán-Sánchez A, Ferreira-Hermosillo A, Ramírez-Rentería C, Luque-de León E, Bosco-Garate I, Laredo-Sánchez F, Contreras-Herrera R, Mac Gregor-Gooch J, Cuevas-García C, Mendoza-Zubieta V. Clinical and biochemical characteristics of patients with morbid obesity at the time of hospital admission and one year after undergoing bariatric surgery. Rev Med Inst Mex Seguro Soc. 2016;54 Suppl 2:S118–S123. - PubMed
-
- Belligoli A, Sanna M, Serra R, Fabris R, Pra' CD, Conci S, Fioretto P, Prevedello L, Foletto M, Vettor R, Busetto L. Incidence and Predictors of Hypoglycemia 1 Year After Laparoscopic Sleeve Gastrectomy. Obes Surg. 2017;27:3179–3186. - PubMed
-
- Guilbert L, Joo P, Ortiz C, Sepúlveda E, Alabi F, León A, Piña T, Zerrweck C. Safety and efficacy of bariatric surgery in Mexico: A detailed analysis of 500 surgeries performed at a high-volume center. Rev Gastroenterol Mex (Engl Ed) 2019;84:296–302. - PubMed
-
- Yang J, Gao Z, Williams DB, Wang C, Lee S, Zhou X, Qiu P. Effect of laparoscopic Roux-en-Y gastric bypass versus laparoscopic sleeve gastrectomy on fasting gastrointestinal and pancreatic peptide hormones: A prospective nonrandomized trial. Surg Obes Relat Dis. 2018;14:1521–1529. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
