

[Clinicopathological features and prognostic analysis of papillary renal cell carcinoma]
- PMID: 35950382
- PMCID: PMC9385512
- DOI: 10.19723/j.issn.1671-167X.2022.04.006
[Clinicopathological features and prognostic analysis of papillary renal cell carcinoma]
Abstract
Objective: To investigate the clinicopathological features and prognostic characteristics of papillary renal cell carcinoma (pRCC).
Methods: The clinical data of 114 patients with pRCC, including 91 males and 23 females, admitted to the Department of Urology, Peking University Third Hospital from May 2012 to May 2021 were retrospectively analyzed. All the cases were operated patients with clear pathological diagnosis and complete follow-up data. The log-rank test was used to analyze the relationship between the patients' clinicopathological characteristics and survival time, the Kaplan-Meier method to draw survival curves, and the Cox regression model for univariate and multifactorial analysis.
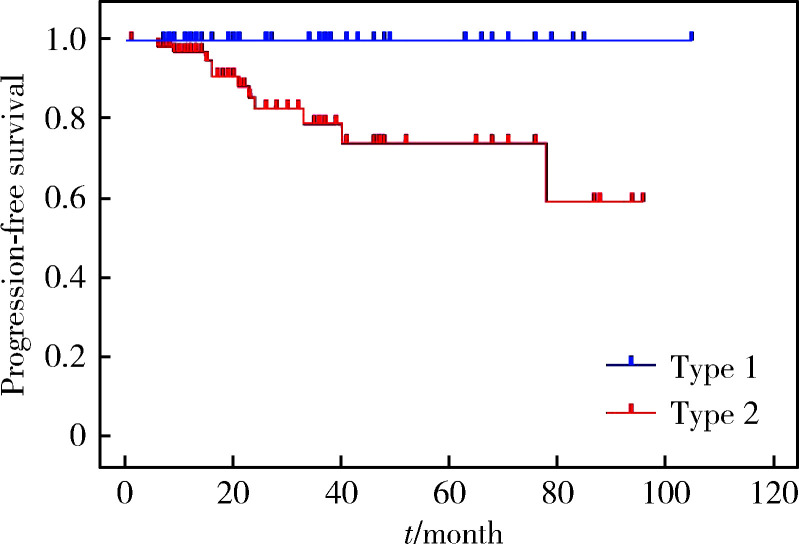
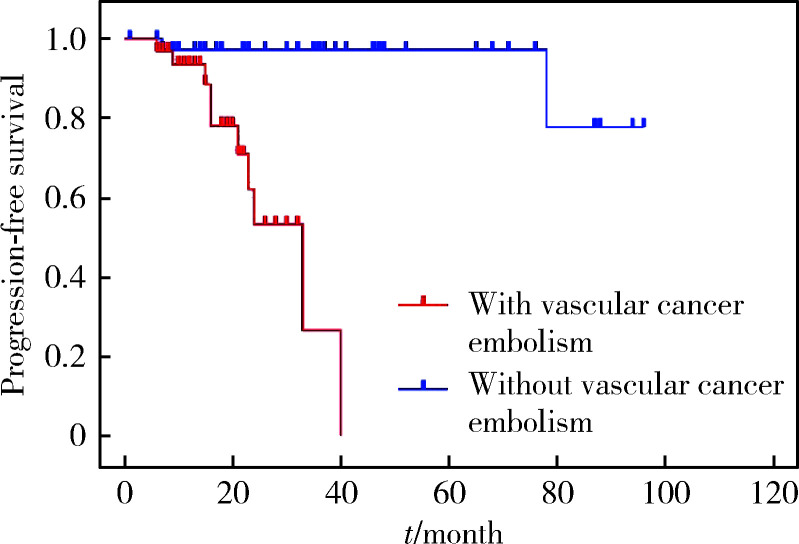
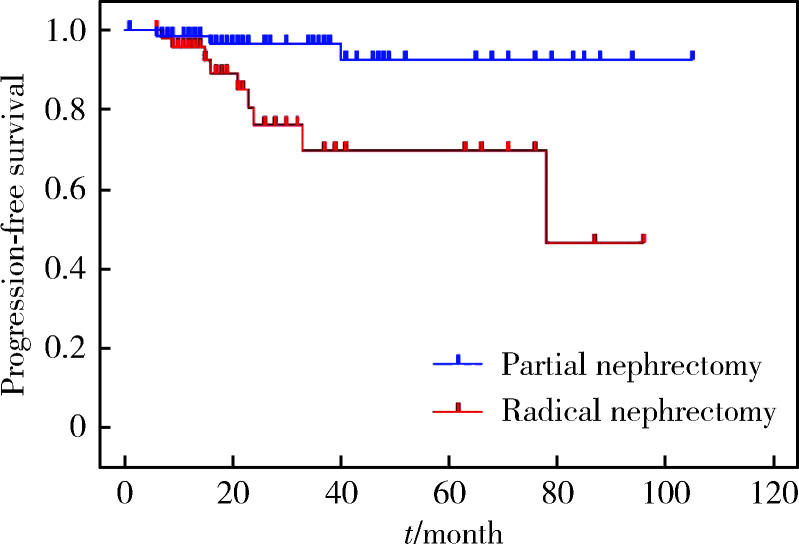
Results: The mean age of the 114 patients was (57.3±12.6) years. The tumors were located in the left kidney in 49 cases and in the right kidney in 65 cases. In the study, 48 radical nephrectomies and 66 partial nephrectomies were performed, 42 cases were type 1 and 72 cases were type 2, and the mean maximum tumor diameter was (5.5±3.6) cm. pT1a stage 52 cases, pT1b stage 22 cases, pT2 stage 4 cases, pT3 stage 33 cases, and pT4 stage 3 cases were staged. According to the World Health Organization / International Society of Urological Pathology (WHO/ISUP), there were 13 cases of gradeⅠ, 44 cases of grade Ⅱ, 51 cases of grade Ⅲ, and 6 cases of grade Ⅳ. And 34 of the 114 patients had vascular cancer embolism, 30 cases had lymph node metastasis, and 3 cases had adrenal metastasis. The median follow-up time after surgery was 22 months, and the 3-year progression-free survival rate was 95.6%. The patients with type 1 and type 2 pRCC showed statistically significant differences in age (P=0.046), body mass index (P=0.008), surgical approach (P=0.001), maximum tumor diameter (P < 0.001), vascular cancer embolism (P < 0.001), lymph node metastasis (P < 0.001), pT stage (P < 0.001), and nuclear grade (P < 0.001). The 3-year progression-free survival rates for type 1 and type 2 pRCC were 100% and 69.4%, respectively, with type 1 having a significantly better prognosis than with type 2 (P=0.003). Univariate analysis of the patients with type 2 pRCC showed that pT stage (P < 0.001), vascular cancer embolism (P < 0.001) and lymph node metastasis (P < 0.001) were strongly associated with their prognosis. Multifactorial analysis showed that vascular cancer embolism was an independent prognostic factor for progression-free survival in type 2 pRCC (P=0.001). Univariate analysis of the pRCC patients undergoing radical nephrectomy showed that pT stage (P=0.006), vascular cancer embolism (P=0.001), and lymph node metastasis (P=0.008) were significant factors affecting their prognosis, and further multifactorial analysis showed that only vascular cancer embolism was an indepen-dent prognostic factor for their progression-free survival (P=0.006).
Conclusion: Type 2 pRCC has more morbidity, more lymph node metastases, more advanced pT stage, and higher pathologic grading than type 1 pRCC. The presence of vascular cancer embolism is an independent prognostic factor in patients with type 2 pRCC and pRCC undergoing radical nephrectomy.
目的: 探讨乳头状肾细胞癌(papillary renal cell carcinoma,pRCC)的临床病理特征和预后特点。
方法: 回顾性分析2012年5月至2021年5月北京大学第三医院泌尿外科收治的114例pRCC患者的临床资料,包括91例男性和23例女性。所有病例均为手术患者,病理诊断明确,随访数据完整。采用Kaplan-Meier法绘制生存曲线并通过log-rank检验分析患者临床病理特征与生存时间的关系,使用Cox比例风险回归模型分析影响患者无进展生存率的因素。
结果: 114例患者平均年龄(57.3±12.6)岁。肿瘤位于左肾49例,右肾65例。48例行根治性肾切除术,66例行肾部分切除术。1型pRCC 42例,2型72例,肿瘤平均最大径为(5.5±3.6) cm。肿瘤分期pT1a期52例,pT1b期22例,pT2期4例,pT3期33例,pT4期3例。2016年世界卫生组织/国际泌尿病理学会(World Health Organization / International Society of Urological Pathology,WHO/ISUP)分级Ⅰ级13例,Ⅱ级44例,Ⅲ级51例,Ⅳ级6例。114例患者中34例伴有脉管癌栓,30例伴淋巴结转移,3例伴肾上腺转移。患者术后中位随访时间为22个月,3年无进展生存率为95.6%。1型和2型pRCC患者在年龄(P=0.046)、体重指数(P=0.008)、手术方式(P=0.001)、肿瘤最大径(P < 0.001)、脉管癌栓(P < 0.001)、淋巴结转移(P < 0.001)、pT分期(P < 0.001)和核分级(P < 0.001)方面差异均有统计学意义。1型和2型pRCC的3年无进展生存率分别为100%和69.4%,1型预后明显优于2型(P=0.003)。2型pRCC患者的单因素分析结果显示,pT分期(P < 0.001)、脉管癌栓(P < 0.001)和淋巴结转移(P < 0.001)与其预后紧密相关;多因素分析显示,脉管癌栓为2型pRCC无进展生存率的独立预后因素(P=0.001)。行根治性肾切除术的pRCC患者的单因素分析结果显示,pT分期(P=0.006)、脉管癌栓(P=0.001)和淋巴结转移(P=0.008)是影响其预后的显著因素,进一步多因素分析显示只有脉管癌栓是其无进展生存率的独立预后因素(P=0.006)。
结论: 2型pRCC比1型pRCC发病率更高,淋巴结转移更易出现,pT分期更晚,核分级更高。在2型pRCC和根治性切除术后的pRCC患者中,脉管癌栓是其独立预后因素。
Keywords: Clinical features; Clinical pathology; Papillary renal cell carcinoma; Prognosis.
Figures
Similar articles
-
Clinicopathological Features and Prognostic Outcomes of Papillary Renal Cell Carcinoma.Int J Gen Med. 2021 Nov 2;14:7523-7531. doi: 10.2147/IJGM.S340569. eCollection 2021. Int J Gen Med. 2021. PMID: 34754225 Free PMC article.
-
The Clinicopathological Features and Prognosis in Patients With Papillary Renal Cell Carcinoma: A Multicenter Retrospective Study in Chinese Population.Front Oncol. 2021 Sep 21;11:753690. doi: 10.3389/fonc.2021.753690. eCollection 2021. Front Oncol. 2021. PMID: 34621685 Free PMC article.
-
[Long-term survival analysis of 1 367 patients treated with radical nephrectomy from a single center].Zhonghua Zhong Liu Za Zhi. 2023 Nov 23;45(11):981-987. doi: 10.3760/cma.j.cn112152-20220614-00420. Zhonghua Zhong Liu Za Zhi. 2023. PMID: 37968085 Chinese.
-
Contemporary review of papillary renal cell carcinoma-current state and future directions.Virchows Arch. 2024 Sep;485(3):391-405. doi: 10.1007/s00428-024-03865-x. Epub 2024 Jul 12. Virchows Arch. 2024. PMID: 38995356 Review.
-
Role of clinicopathological variables in predicting recurrence and survival outcomes after surgery for non-metastatic renal cell carcinoma: Systematic review and meta-analysis.Int J Cancer. 2024 Apr 1;154(7):1309-1323. doi: 10.1002/ijc.34793. Epub 2023 Nov 27. Int J Cancer. 2024. PMID: 38009868
Cited by
-
[Clinicopathologic features and prognosis of young renal tumors with tumor thrombus].Beijing Da Xue Xue Bao Yi Xue Ban. 2023 Oct 18;55(5):802-811. doi: 10.19723/j.issn.1671-167X.2023.05.005. Beijing Da Xue Xue Bao Yi Xue Ban. 2023. PMID: 37807732 Free PMC article. Chinese.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical