

[Correlation between metabolic syndrome and prognosis of patients with clear cell renal cell carcinoma]
- PMID: 35950385
- PMCID: PMC9385524
- DOI: 10.19723/j.issn.1671-167X.2022.04.009
[Correlation between metabolic syndrome and prognosis of patients with clear cell renal cell carcinoma]
Abstract
Objective: To investigate the effects of MetS on the prognosis of patients with clear cell renal cell carcinoma (ccRCC).
Methods: Clinical and pathological data and the laboratory test of ccRCC 342 patients with diverticular stones who underwent ccRCC who underwent radical or partial nephrectomy were retrospectively collected and analyzed.The patients were divided into MetS group and non-MetS group, and the subgroups were defined according to the tumor size. The overall survival (OS), cancer-specific survival (CSS), and progression-free survival (PFS) of the two groups were analyzed by univariate Cox analysis, and the subgroup analyses were also performed. Kaplan-Meier survival curve and survival analysis for OS, CSS, and PFS of the two groups and the subgroups were conducted.
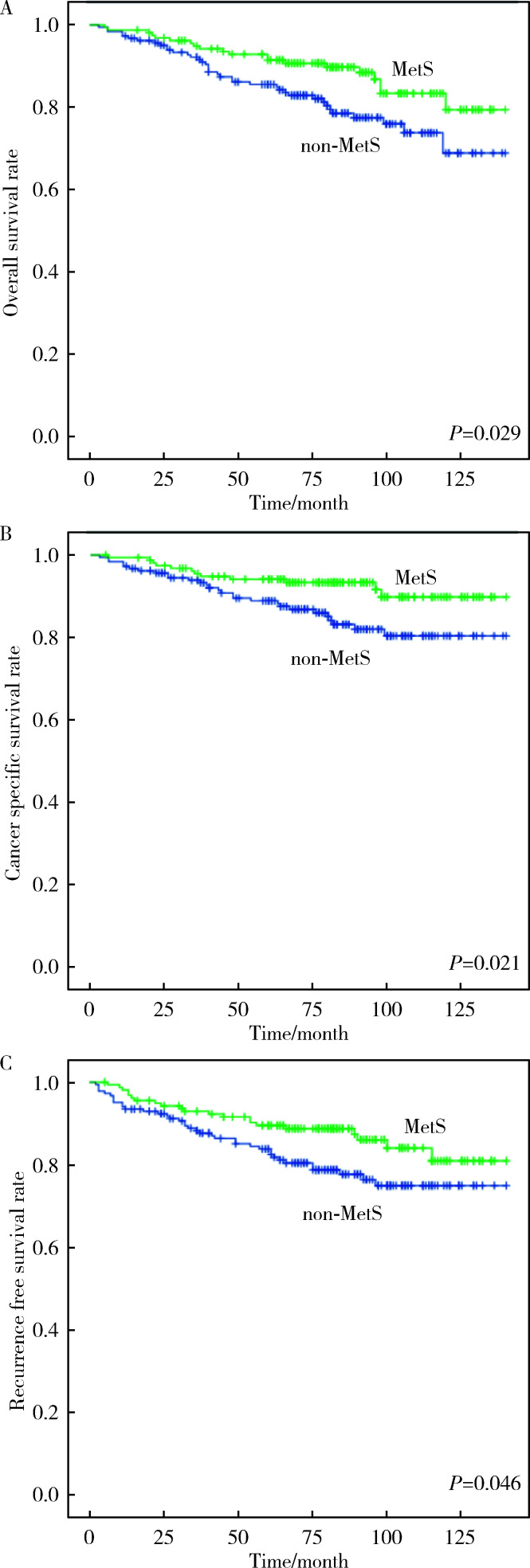
Results: Univariate Cox analysis showed that MetS was a protective factor of postoperative OS [hazard ratio (HR)=0.551, 95%CI: 0.321-0.949, P=0.031], CSS (HR=0.460, 95%CI: 0.234-0.905, P=0.025), and PFS (HR 0.585, 95%CI: 0.343-0.998, P=0.049) in the patients with ccRCC. In the subgroup with tumor size≤4 cm, MetS was not associated with postoperative OS (HR=0.857, 95%CI: 0.389-1.890, P=0.702), CSS (HR=1.129, 95%CI: 0.364-3.502, P=0.833), and PFS (HR=1.554, 95%CI: 0.625-3.864, P=0.343). In the subgroup with tumor size>4 cm, Mets was a protective factor of postoperative OS (HR=0.377, 95%CI: 0.175-0.812, P=0.013), CSS (HR=0.280, 95%CI: 0.113-0.690, P=0.006), and PFS (HR=0.332, 95%CI: 0.157-0.659, P=0.002); Obesity was a protective factor of postoperative CSS (HR=0.464, 95%CI: 0.219-0.981, P=0.044), and PFS (HR=0.445, 95%CI: 0.238-0.833, P=0.011). Kaplan-Meier survival analysis showed that the long-term survival of patients with MetS was better than those without MetS in OS (P=0.029), CSS (P=0.021), and PFS (P=0.046); for the subgroup with tumor size≤4 cm, there was no significant difference in postoperative OS (P=0.702), CSS (P=0.833), and PFS (P=0.339) between patients with and without MetS; For the subgroup with tumor size>4 cm, the OS (P=0.010), CSS (P=0.003), and PFS (P=0.001) of patients with MetS were better than those without MetS.
Conclusion: MetS was a protective factor of postoperative OS, CSS, and PFS in the patients with ccRCC, which was more obvious in subgroup with tumor size>4 cm. And obesity, the component of MetS, was correlated with postoperative OS and CSS.
目的: 探讨肾透明细胞癌(clear cell renal cell carcinoma,ccRCC)手术后患者中代谢综合征(metabolic syndrome,MetS)与ccRCC预后的相关性。
方法: 选择2009年1月—2014年11月于北京大学人民医院行根治性肾切除术或部分肾切除术患者的病例资料进行回顾性分析,共收集到342例ccRCC患者,记录患者的临床资料和病理资料,以及治疗前的实验室检查结果。将患者分为合并MetS组及未合并MetS组,对两组患者的总生存期(overall survival,OS)、肿瘤特异性生存期(cancer-specific survival,CSS)和无进展生存期(progression-free survival,PFS)进行单变量Cox回归分析与亚组分析。对两组患者以及各亚组的OS、CSS以及PFS使用Kaplan-Meier法绘制生存曲线进行生存分析。
结果: 单变量Cox回归分析发现,MetS是ccRCC术后OS [风险比(hazard ratio,HR)=0.551,95%CI:0.321~0.949,P=0.031]、CSS(HR=0.460,95%CI 0.234~0.905,P=0.025)以及PFS(HR=0.585,95%CI:0.343~0.998,P=0.049)的保护因素。在肿瘤直径≤4 cm的亚组,MetS与术后OS(HR= 0.857,95%CI:0.389~1.890,P=0.702)、CSS(HR=1.129,95%CI:0.364~3.502,P=0.833)以及PFS(HR=1.554,95%CI:0.625~3.864,P=0.343)无明显相关性。在肿瘤直径>4 cm的亚组,MetS是ccRCC术后OS(HR=0.377,95%CI:0.175~0.812,P=0.013)、CSS(HR=0.280,95%CI:0.113~0.690,P=0.006)以及PFS(HR=0.332,95%CI:0.157~0.659,P=0.002)的保护因素;肥胖是术后CSS(HR=0.464,95%CI:0.219~0.981,P=0.044)和PFS(HR=0.445,95%CI:0.238~0.833,P=0.011)的保护因素。Kaplan-Meier生存分析显示,合并MetS较未合并MetS的患者术后远期生存更佳,二者OS(P=0.029)、CSS(P=0.021)以及PFS(P=0.046)差异均具有统计学意义;对肿瘤直径≤4 cm的亚组,合并MetS与未合并MetS的ccRCC患者术后OS(P=0.702)、CSS(P=0.833)以及PFS(P=0.339)差异均无统计学意义;对肿瘤直径> 4 cm的亚组,合并MetS的患者OS(P=0.010)、CSS(P=0.003)以及PFS(P=0.001)均高于未合并MetS的患者。
结论: MetS是ccRCC患者术后OS、CSS和PFS的保护因素,该现象在肿瘤直径>4 cm亚组中更为显著;MetS的组分中肥胖与ccRCC术后OS以及CSS相关。
Keywords: Cancer-specific survival; Clear cell renal cell carcinoma; Metabolic syndrome; Overall survival; Progression-free survival.
Figures

Similar articles
-
Influence of metabolic syndrome on survival of patients with localized renal clear cell carcinoma: A retrospective cohort study in China.Urol Oncol. 2023 May;41(5):257.e19-257.e26. doi: 10.1016/j.urolonc.2023.01.023. Epub 2023 Mar 24. Urol Oncol. 2023. PMID: 36967252
-
Metabolic Syndrome Negatively Impacts the Outcome of Localized Renal Cell Carcinoma.Horm Cancer. 2017 Apr;8(2):127-134. doi: 10.1007/s12672-017-0289-2. Epub 2017 Feb 28. Horm Cancer. 2017. PMID: 28247362 Free PMC article.
-
Does chromophobe renal cell carcinoma have better survival than clear cell renal cell carcinoma? A clinical-based cohort study and meta-analysis.Int Urol Nephrol. 2016 Feb;48(2):191-9. doi: 10.1007/s11255-015-1161-3. Epub 2015 Nov 20. Int Urol Nephrol. 2016. PMID: 26589610 Review.
-
Multicenter Study of Controlling Nutritional Status (CONUT) Score as a Prognostic Factor in Patients With HIV-Related Renal Cell Carcinoma.Front Immunol. 2021 Nov 30;12:778746. doi: 10.3389/fimmu.2021.778746. eCollection 2021. Front Immunol. 2021. PMID: 34917092 Free PMC article.
-
High Ki-67 Immunohistochemical Reactivity Correlates With Poor Prognosis in Bladder Carcinoma: A Comprehensive Meta-Analysis with 13,053 Patients Involved.Medicine (Baltimore). 2016 Apr;95(15):e3337. doi: 10.1097/MD.0000000000003337. Medicine (Baltimore). 2016. PMID: 27082587 Free PMC article. Review.
Cited by
-
Metabolic syndrome and increased susceptibility to renal cell carcinoma - a meta-analysis.BMC Nephrol. 2025 Feb 26;26(1):102. doi: 10.1186/s12882-025-04013-6. BMC Nephrol. 2025. PMID: 40012054 Free PMC article.
References
-
-
Chakiryan NH, Jiang DD, Gillis KA, et al. Real-world survival outcomes associated with first-line immunotherapy, targeted therapy, and combination therapy for metastatic clear cell renal cell carcinoma[J]. JAMA Netw Open, 2021, 4(5): e2111329[2022-03-01]. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8150693/.
-
MeSH terms
LinkOut - more resources
Full Text Sources
Medical