

Tumor Grade Predicts for Calcitonin Doubling Times and Disease-Specific Outcomes After Resection of Medullary Thyroid Carcinoma
- PMID: 35950622
- PMCID: PMC9595606
- DOI: 10.1089/thy.2022.0217
Tumor Grade Predicts for Calcitonin Doubling Times and Disease-Specific Outcomes After Resection of Medullary Thyroid Carcinoma
Abstract
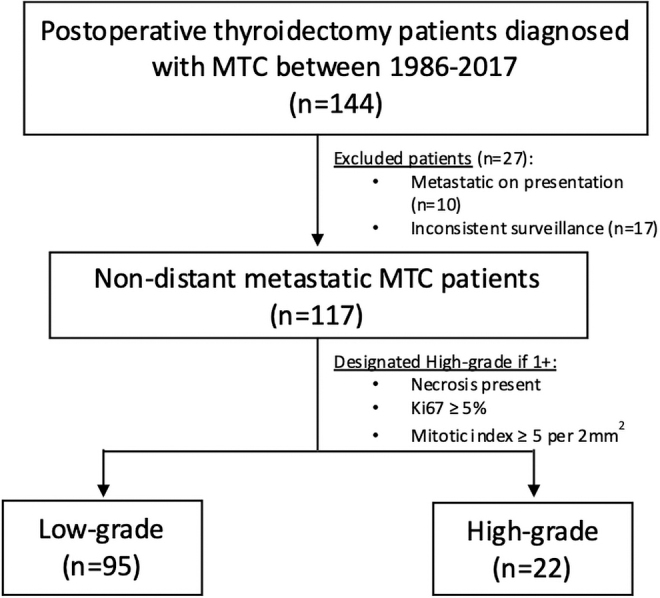
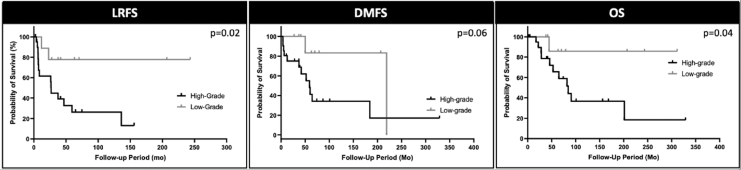
Background: Tumor grade is a new validated prognostic factor for medullary thyroid cancer (MTC). Calcitonin doubling time can predict MTC recurrence. We aimed to describe the association of tumor grade with calcitonin doubling and its effect on disease-specific outcomes times after resection. Methods: A retrospective analysis of MTC patients who underwent resection at a single tertiary-care cancer center between 1986 and 2017 were evaluated. Tumors were designated as high-grade MTC if two head and neck pathologists identified mitotic index ≥5 per 2 mm2, tumor necrosis, or a Ki67 proliferative index ≥5% within the tumor. Calcitonin doubling time was calculated using a validated calculator with at least three consecutive levels. Using Cox proportional hazards models, outcomes evaluated included locoregional relapse-free survival (LRFS), distant metastasis-free survival (DMFS), and overall survival (OS). Results: Among 117 patients, 95 were low grade and 22 high grade. Median follow-up was 70.2 months. High-grade patients demonstrated significantly faster calcitonin doubling times when compared with low-grade patients (8.51 ± 3.22 months vs. 38.42 ± 11.19 months; p < 0.001). In addition, most high-grade patients (66.7%) had calcitonin doubling times less than 1 year compared with fewer low-grade patients (1.0%; p < 0.001). High- and low-grade patients were further stratified by those who had calcitonin doubling times less than or greater than 2 years-a previously validated prognostic cutoff point. For patients with calcitonin doubling times less than 2 years, 70% were high grade, while 30% were low grade (p < 0.001). On multivariate analysis comparing grade and calcitonin doubling times, high-grade patients had significantly worse LRFS (hazards ratio [HR] 4.77 [confidence interval; CI 1.19-8.81]), DMFS (HR 7.25 [CI 2.36-22.28]), and OS (HR 6.04 [CI 1.85-19.72]; p < 0.05 for all), while calcitonin doubling times less than 2 years had worse DMFS (HR 7.22 [CI 1.05-49.75]). High-grade patients with calcitonin doubling times less than 2 years had associated worse LRFS and OS (both p < 0.05) compared with low-grade patients. Conclusions: The majority of high-grade MTC patients have calcitonin doubling times less than 2years. Close monitoring should be advocated for patients assessed to have high-grade tumors as they are at risk for poor disease-specific outcomes and structural recurrence.
Keywords: IMTCGS; MTC grading; MTC surveillance; calcitonin doubling times; medullary thyroid carcinoma.
Conflict of interest statement
No competing financial interests exist.
Figures
Similar articles
-
The Usefulness of the International Grading System in the Management of Sporadic Medullary Thyroid Carcinoma.Thyroid. 2025 Apr;35(4):387-396. doi: 10.1089/thy.2024.0444. Epub 2025 Feb 11. Thyroid. 2025. PMID: 39930944
-
International medullary thyroid carcinoma grading system: an Indian tertiary care centre experience.Eur Arch Otorhinolaryngol. 2024 Mar;281(3):1571-1579. doi: 10.1007/s00405-023-08341-x. Epub 2023 Nov 27. Eur Arch Otorhinolaryngol. 2024. PMID: 38010402
-
Independent Validation of the International Grading System for Medullary Thyroid Carcinoma: A Single Institution Experience.Mod Pathol. 2023 Sep;36(9):100235. doi: 10.1016/j.modpat.2023.100235. Epub 2023 Jun 1. Mod Pathol. 2023. PMID: 37270155 Free PMC article.
-
Long-Term Follow-up in Medullary Thyroid Carcinoma.Recent Results Cancer Res. 2015;204:207-25. doi: 10.1007/978-3-319-22542-5_10. Recent Results Cancer Res. 2015. PMID: 26494391 Review.
-
Update on C-Cell Neuroendocrine Neoplasm: Prognostic and Predictive Histopathologic and Molecular Features of Medullary Thyroid Carcinoma.Endocr Pathol. 2023 Mar;34(1):1-22. doi: 10.1007/s12022-023-09753-5. Epub 2023 Mar 8. Endocr Pathol. 2023. PMID: 36890425 Review.
Cited by
-
Early postoperative calcitonin-to-preoperative calcitonin ratio as a predictive marker for structural recurrence in sporadic medullary thyroid cancer: A retrospective study.Front Endocrinol (Lausanne). 2022 Dec 16;13:1094242. doi: 10.3389/fendo.2022.1094242. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36589824 Free PMC article.
-
The 2024 revised clinical guidelines on the management of thyroid tumors by the Japan Association of Endocrine Surgery.Endocr J. 2025 May 7;72(5):545-635. doi: 10.1507/endocrj.EJ24-0644. Epub 2025 Mar 8. Endocr J. 2025. PMID: 40058844 Free PMC article.
-
Management of Medullary Thyroid Cancer: Patterns of Recurrence and Outcomes of Reoperative Surgery.Oncologist. 2023 Dec 11;28(12):1064-1071. doi: 10.1093/oncolo/oyad232. Oncologist. 2023. PMID: 37632760 Free PMC article.
-
A Competing Risk Nomogram for Prediction of Prognosis in Patients With Primary Squamous Cell Thyroid Carcinoma.Technol Cancer Res Treat. 2024 Jan-Dec;23:15330338241254059. doi: 10.1177/15330338241254059. Technol Cancer Res Treat. 2024. PMID: 38725285 Free PMC article.
-
Management of medullary thyroid cancer based on variation of carcinoembryonic antigen and calcitonin.Front Endocrinol (Lausanne). 2024 Oct 10;15:1418657. doi: 10.3389/fendo.2024.1418657. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39449744 Free PMC article. Review.
References
-
- Modigliani E, Cohen R, Campos JM, et al. . Prognostic factors for survival and for biochemical cure in medullary thyroid carcinoma: Results in 899 patients. The GETC Study Group. Groupe d'etude des tumeurs a calcitonine. Clin Endocrinol (Oxf) 1998;48(3):265–273; doi: 10.1046/j.1365-2265.1998.00392.x. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
