

Targeting Plk1 Sensitizes Pancreatic Cancer to Immune Checkpoint Therapy
- PMID: 35950917
- PMCID: PMC9532376
- DOI: 10.1158/0008-5472.CAN-22-0018
Targeting Plk1 Sensitizes Pancreatic Cancer to Immune Checkpoint Therapy
Abstract
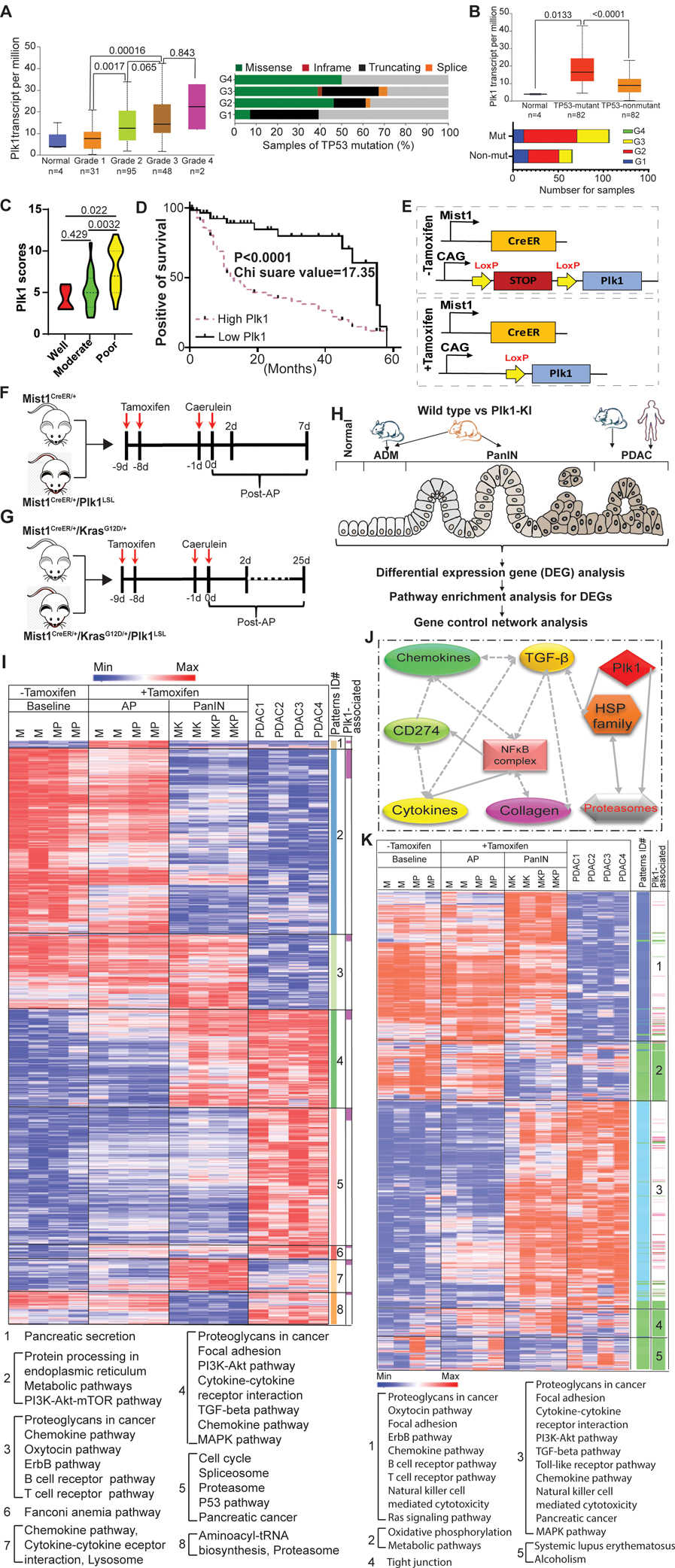
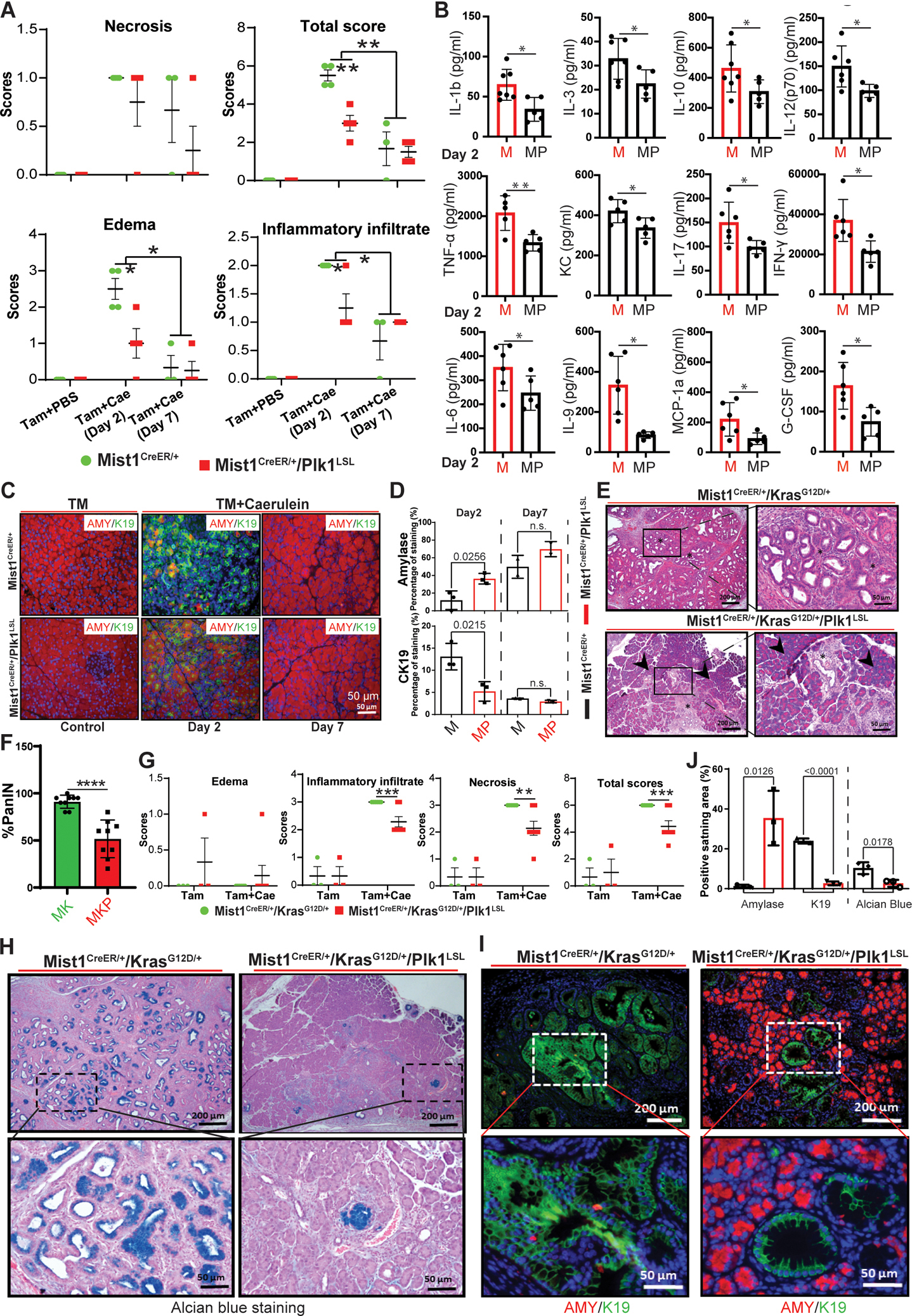
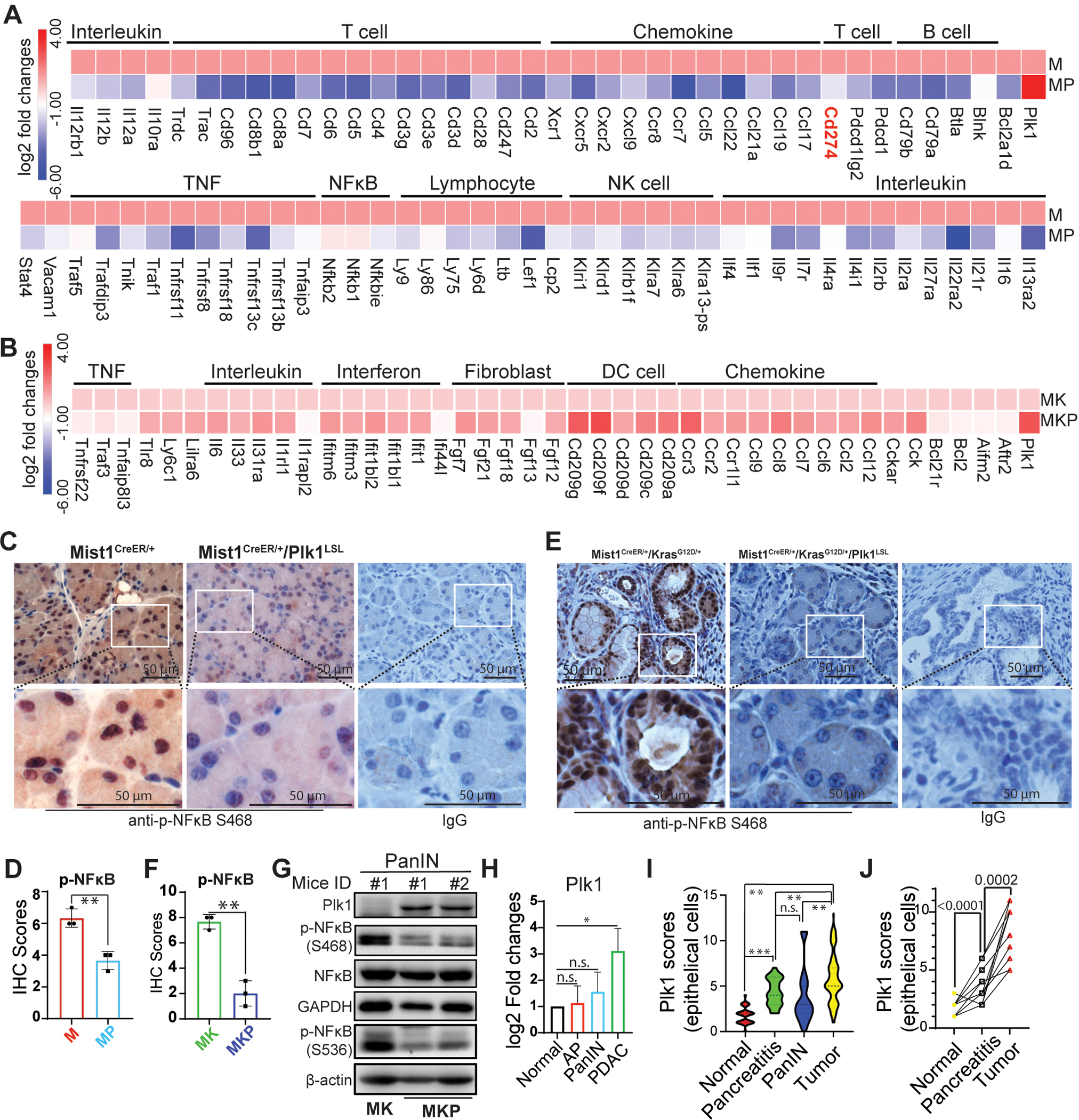
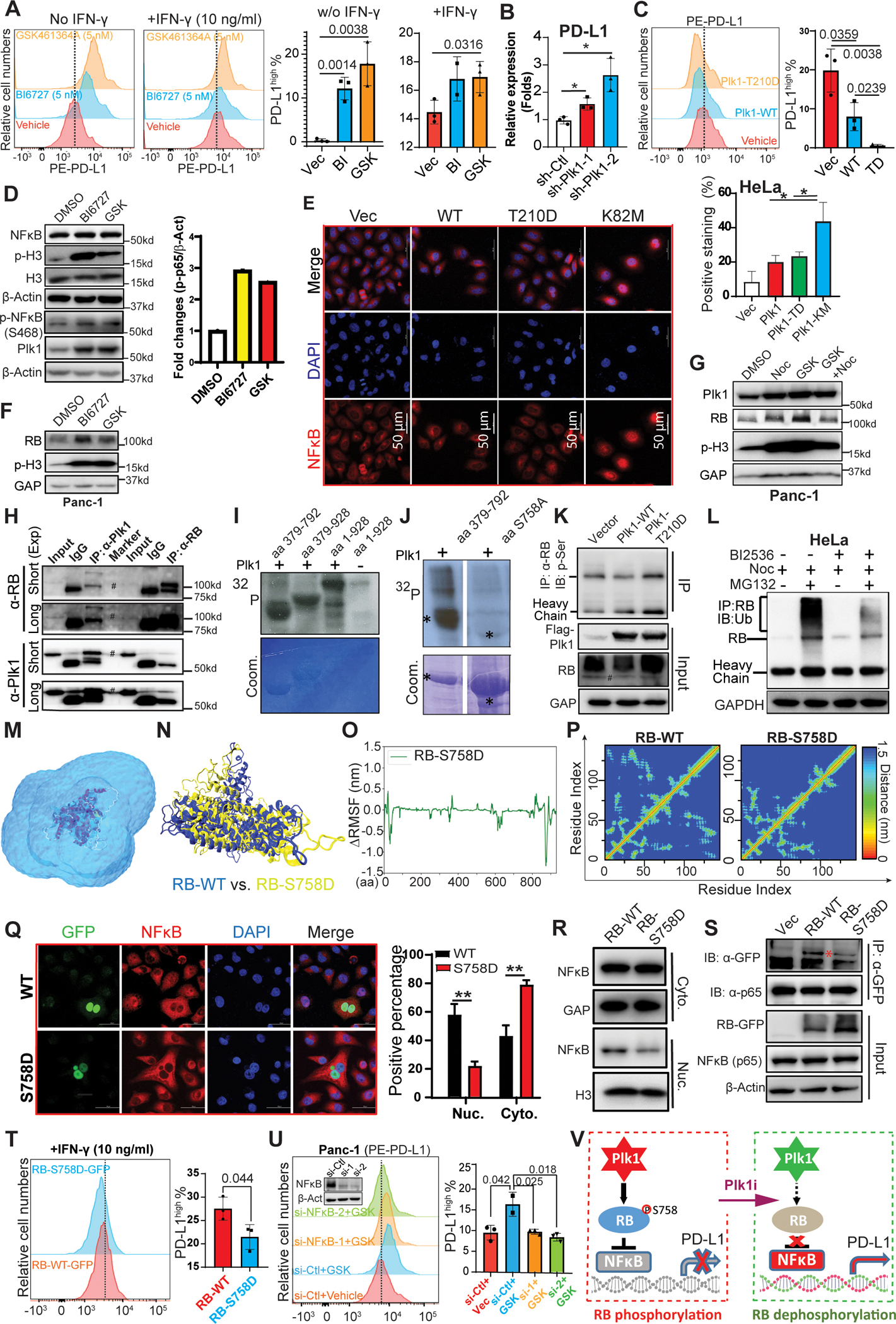
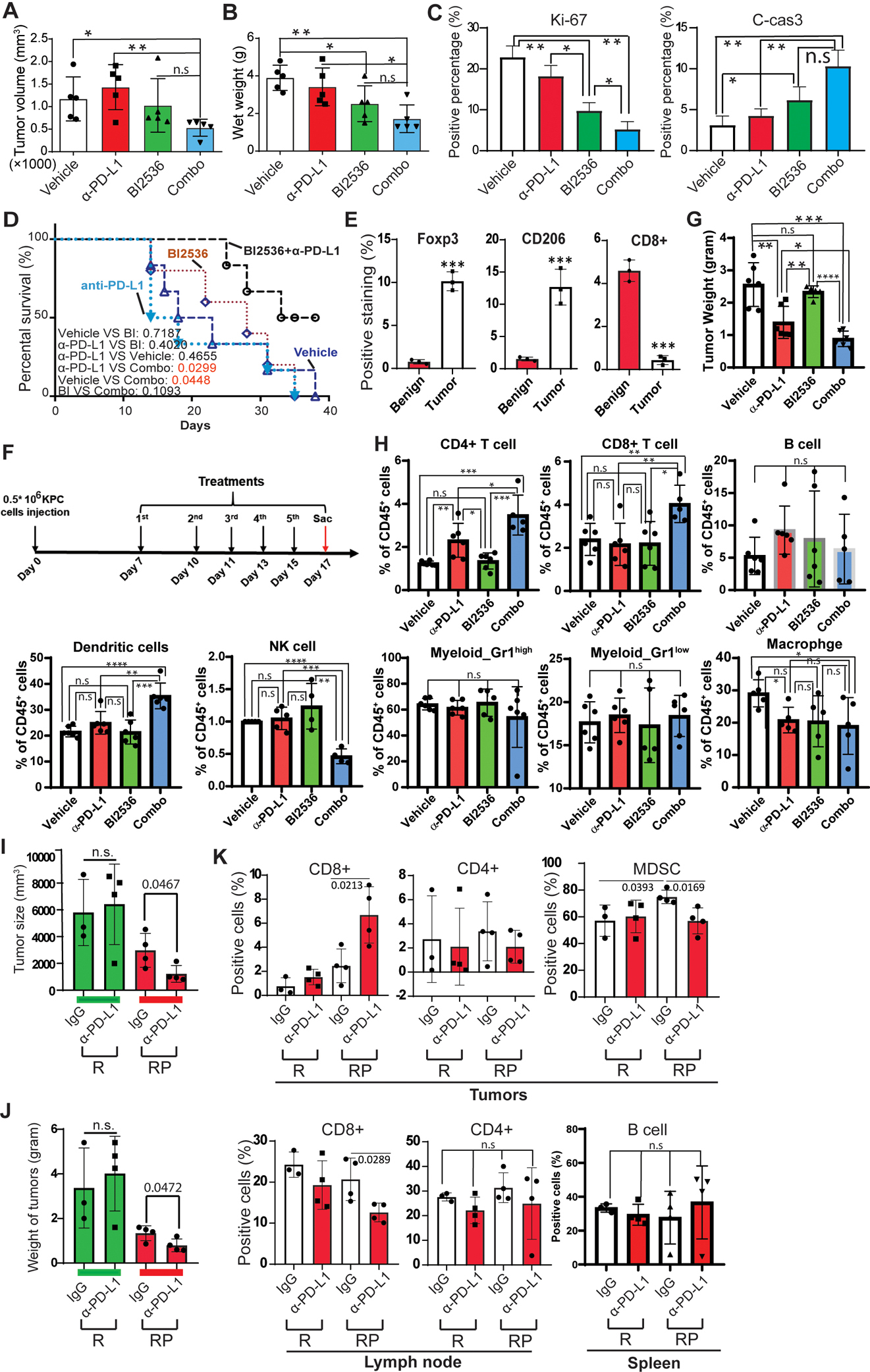
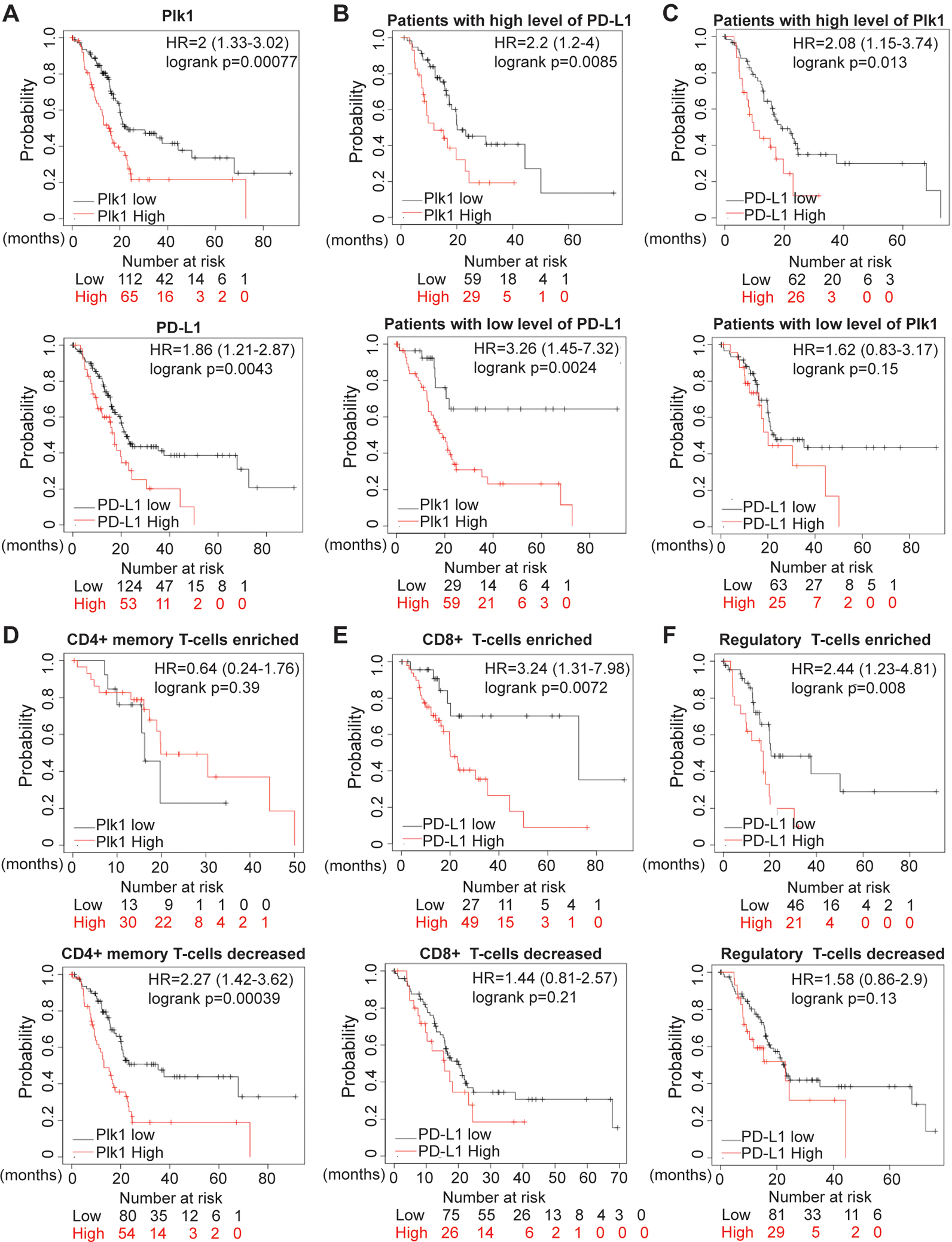
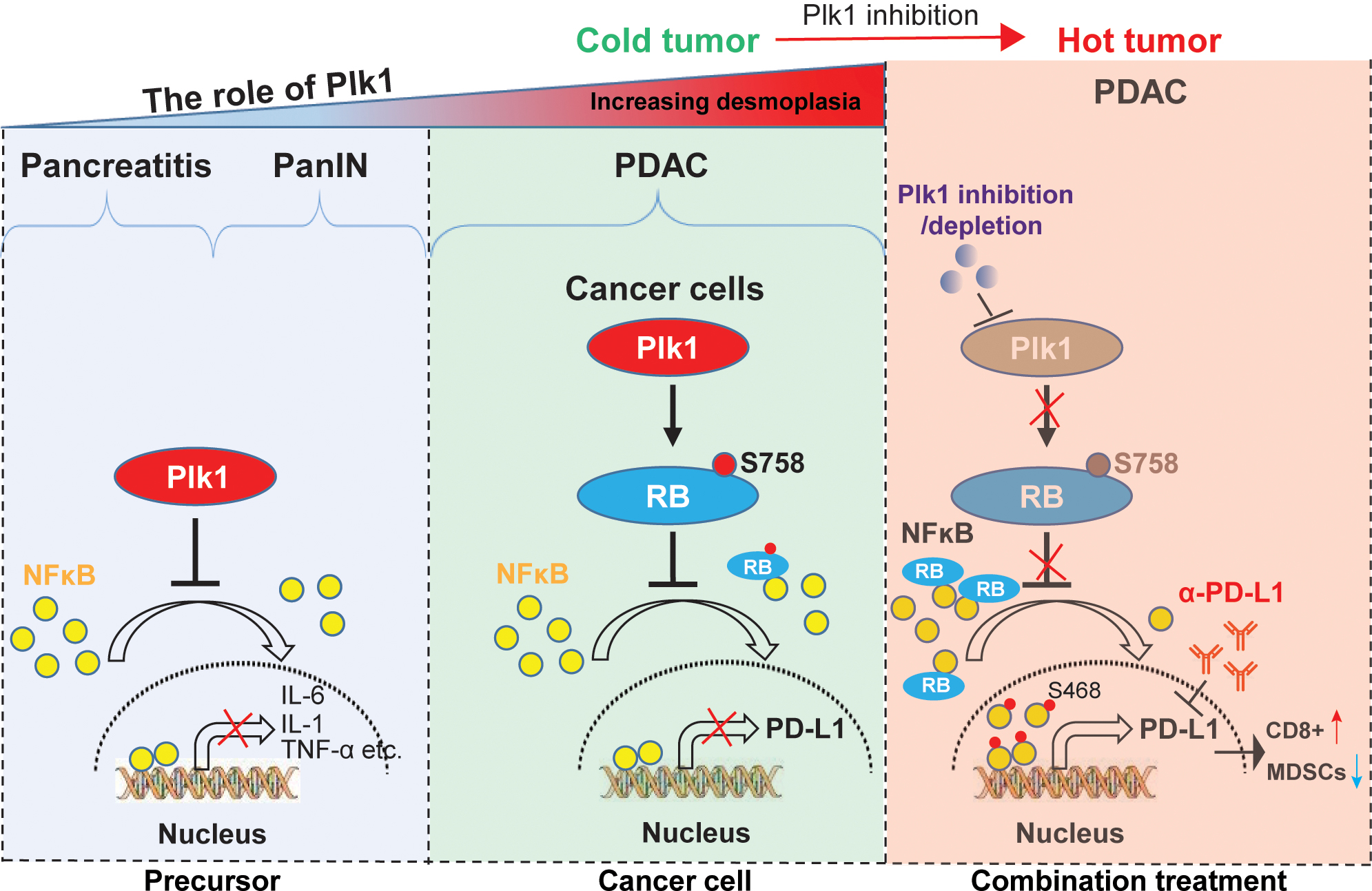
Polo-like kinase 1 (Plk1) plays an important role in cell-cycle regulation. Recent work has suggested that Plk1 could be a biomarker of gemcitabine response in pancreatic ductal adenocarcinoma (PDAC). Although targeting Plk1 to treat PDAC has been attempted in clinical trials, the results were not promising, and the mechanisms of resistance to Plk1 inhibition is poorly understood. In addition, the role of Plk1 in PDAC progression requires further elucidation. Here, we showed that Plk1 was associated with poor outcomes in patients with PDAC. In an inducible transgenic mouse line with specific expression of Plk1 in the pancreas, Plk1 overexpression significantly inhibited caerulein-induced acute pancreatitis and delayed development of acinar-to-ductal metaplasia and pancreatic intraepithelial neoplasia. Bioinformatics analyses identified the regulatory networks in which Plk1 is involved in PDAC disease progression, including multiple inflammation-related pathways. Unexpectedly, inhibition or depletion of Plk1 resulted in upregulation of PD-L1 via activation of the NF-κB pathway. Mechanistically, Plk1-mediated phosphorylation of RB at S758 inhibited the translocation of NF-κB to nucleus, inactivating the pathway. Inhibition of Plk1 sensitized PDAC to immune checkpoint blockade therapy through activation of an antitumor immune response. Together, Plk1 suppresses PDAC progression and inhibits NF-κB activity, and targeting Plk1 can potentiate the efficacy of immunotherapy in PDAC.
Significance: Inhibition of Plk1 induces upregulation of PD-L1 expression in pancreatic ductal adenocarcinoma, stimulating antitumor immunity and sensitizing tumors to immunotherapy.
©2022 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA Cancer J Clin 2021;71:7–33 - PubMed
-
- Seton-Rogers S Tumorigenesis: Pushing pancreatic cancer to take off. Nat Rev Cancer 2012;12:739. - PubMed
-
- Mizrahi JD, Surana R, Valle JW, Shroff RT. Pancreatic cancer. Lancet 2020;395:2008–20 - PubMed
-
- Strebhardt K Multifaceted polo-like kinases: drug targets and antitargets for cancer therapy. Nat Rev Drug Discov 2010;9:643–60 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
