

Left atrial appendage sealing performance of the Amplatzer Amulet and Watchman FLX device
- PMID: 35951214
- PMCID: PMC9977851
- DOI: 10.1007/s10840-022-01336-4
Left atrial appendage sealing performance of the Amplatzer Amulet and Watchman FLX device
Erratum in
-
Correction to: Left atrial appendage sealing performance of the Amplatzer Amulet and Watchman FLX device.J Interv Card Electrophysiol. 2023 Mar;66(2):403. doi: 10.1007/s10840-022-01397-5. J Interv Card Electrophysiol. 2023. PMID: 36269470 Free PMC article. No abstract available.
Abstract
Background: The left atrial appendage (LAA) sealing properties of the Amplatzer Amulet and Watchman FLX devices were compared using cardiac computed tomography (CT) follow-up.
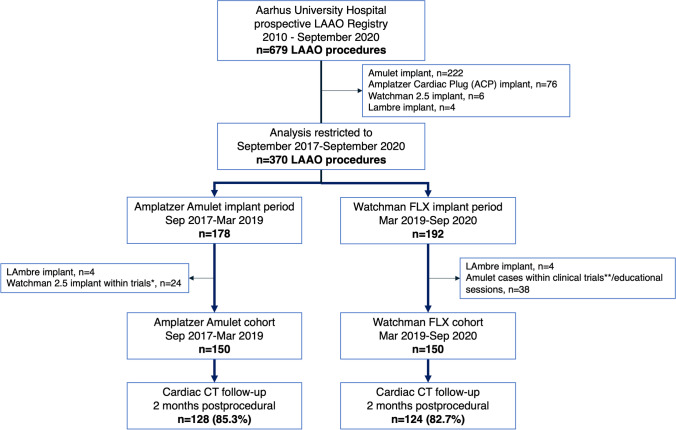
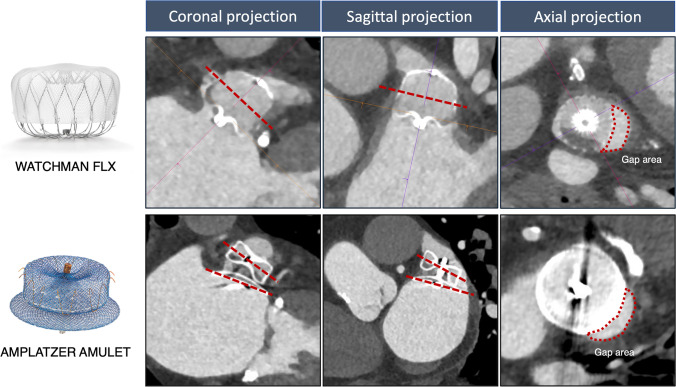
Methods: Single-center cohort study of patients undergoing LAAO between 2017 and 2020. Two consecutive cohorts were enrolled, one treated with the Amplatzer Amulet (n = 150) up till 2019, and a second cohort treated with the Watchman FLX (n = 150) device from 2019. Cardiac CT was performed 2 months postprocedure. The primary outcome was complete LAA occlusion defined as no visible peri-device leak (PDL) and absence of contrast patency in the distal LAA. Secondary outcomes included PDL, contrast patency without visible PDL, PDL area, and periprocedural complications.
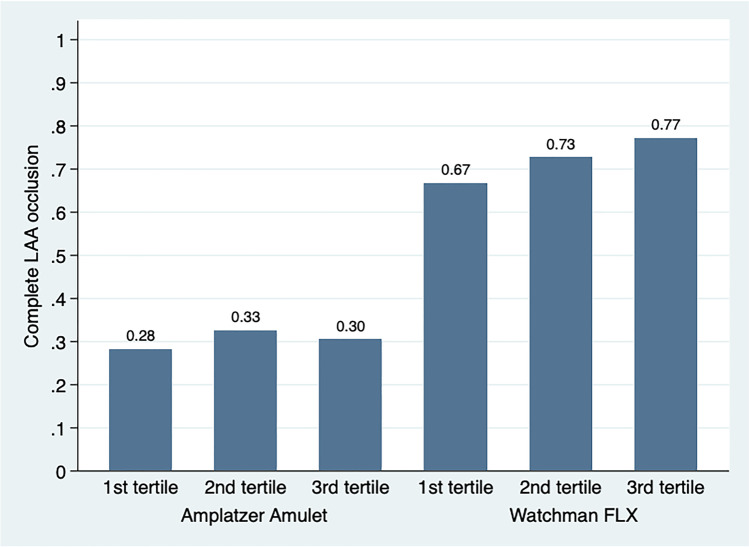
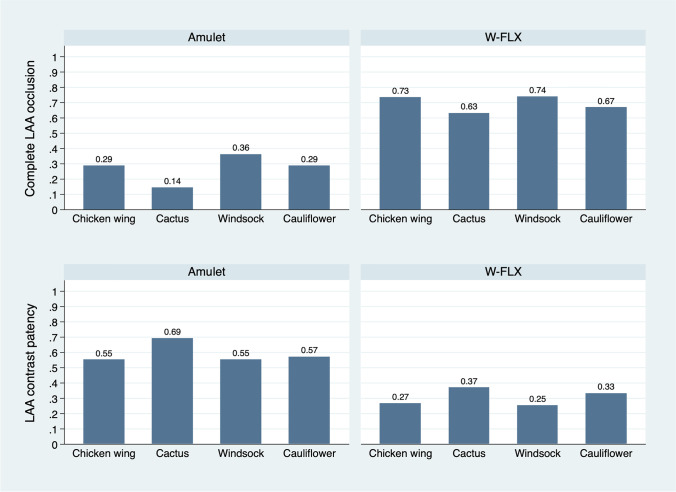
Results: Complete occlusion was achieved in 39 (30.5%) of the Amulet group, compared to 89 (71.8%) of the FLX group, p < 0.001. A PDL at the Amulet disc was present in 65 (50.8%), at the lobe in 16 (12.5%), and at both the disc and lobe in 13 (10.2%). For FLX, a PDL was present in 20 (16.1%). Contrast patency without visible PDL was observed in 24 (18.8%) and 15 (12.1%) of the Amulet and FLX group, respectively. The PDL area at the Amulet mid-lobe was 92 mm2 (59-158) and 32 mm2 (IQR 28-96) for FLX, p = 0.019. Device-related thrombosis occurred in 1 (0.7%) and 2 (1.3%), respectively (p = 0.99), with periprocedural adverse events occurring in 6 (4%) and 8 (5.3%) of the Amulet and FLX group (p = 0.79).
Conclusion: Complete LAA occlusion was achieved in a significantly higher proportion treated with the Watchman FLX compared to the Amulet device. PDL was smaller with the FLX than the Amulet. Conceptual device design differences make interpretation of results complex, and additional studies with clinical outcomes are needed.
Keywords: Amulet; Atrial fibrillation; Computed tomography; Left atrial appendage occlusion; Watchman.
© 2022. The Author(s).
Conflict of interest statement
Dr. Korsholm has received lecture fees from Boston Scientific and Abbott. Dr. Andersen has received consulting fees from Boston Scientific. Dr. Nielsen-Kudsk is proctor for Boston Scientific and Abbott. The remaining authors have nothing to disclosure in relation to the present work.
Figures
Comment in
-
Left atrial appendage occlusion: does it get the seal of approval?J Interv Card Electrophysiol. 2023 Mar;66(2):253-254. doi: 10.1007/s10840-022-01381-z. Epub 2022 Sep 28. J Interv Card Electrophysiol. 2023. PMID: 36169789 No abstract available.
Similar articles
-
One year outcome and analysis of peri-device leak of left atrial appendage occlusion devices.J Interv Card Electrophysiol. 2022 Jun;64(1):27-34. doi: 10.1007/s10840-021-01002-1. Epub 2021 May 17. J Interv Card Electrophysiol. 2022. PMID: 34002319 Clinical Trial.
-
Outcomes of Left Atrial Appendage Occlusion Treatment With Amulet After Unsuccessful Watchman FLX Device: A Multicenter Observational Study.J Cardiovasc Electrophysiol. 2025 Jul;36(7):1632-1642. doi: 10.1111/jce.16729. Epub 2025 May 19. J Cardiovasc Electrophysiol. 2025. PMID: 40390276
-
Quantitative considerations for choosing between Amulet and Watchman FLX and management of device related complications.J Interv Card Electrophysiol. 2025 Jun;68(4):909-920. doi: 10.1007/s10840-025-02011-0. Epub 2025 Feb 12. J Interv Card Electrophysiol. 2025. PMID: 39939509
-
Safety and efficacy of percutaneous Watchman 2.5 device versus Amplatzer Amulet for left atrial appendage closure in patients with non-valvular atrial fibrillation: A systematic review and study-level meta-analysis.PLoS One. 2024 Feb 14;19(2):e0295804. doi: 10.1371/journal.pone.0295804. eCollection 2024. PLoS One. 2024. PMID: 38354181 Free PMC article.
-
Clinical efficacy and safety comparison of Watchman device versus ACP/Amulet device for percutaneous left atrial appendage closure in patients with nonvalvular atrial fibrillation: A study-level meta-analysis of clinical trials.Clin Cardiol. 2023 Feb;46(2):117-125. doi: 10.1002/clc.23956. Epub 2022 Nov 30. Clin Cardiol. 2023. PMID: 36448417 Free PMC article. Review.
Cited by
-
Comparative Assessment of Percutaneous Left-Atrial Appendage Occlusion (LAAO) Devices-A Single Center Cohort Study.J Cardiovasc Dev Dis. 2024 May 21;11(6):158. doi: 10.3390/jcdd11060158. J Cardiovasc Dev Dis. 2024. PMID: 38921657 Free PMC article.
-
Comparative Endothelialization of the Watchman Plug Device and LACBES Pacifier Occluder after Left Atrial Appendage Closure.Rev Cardiovasc Med. 2024 Dec 23;25(12):450. doi: 10.31083/j.rcm2512450. eCollection 2024 Dec. Rev Cardiovasc Med. 2024. PMID: 39742236 Free PMC article.
-
Percutaneous left atrial appendage closure for stroke prevention: current challenges and future perspectives.Clin Res Cardiol. 2025 Feb 27. doi: 10.1007/s00392-025-02624-5. Online ahead of print. Clin Res Cardiol. 2025. PMID: 40014086 Review.
-
Clinical outcome and intraprocedural characteristics of left atrial appendage occlusion: a comparison between single-occlusive plug-type and dual-occlusive disc-type devices.Front Cardiovasc Med. 2024 Jul 18;11:1401974. doi: 10.3389/fcvm.2024.1401974. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39091357 Free PMC article.
-
Safety and feasibility of atrial fibrillation ablation after left atrial appendage closure: A single-center experience of the left atrial appendage closure first strategy.J Arrhythm. 2024 May 23;40(4):879-890. doi: 10.1002/joa3.13073. eCollection 2024 Aug. J Arrhythm. 2024. PMID: 39139871 Free PMC article.
References
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomstrom-Lundqvist C, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(5):373–498. doi: 10.1093/eurheartj/ehaa612. - DOI - PubMed
-
- Osmancik P, Herman D, Neuzil P, Hala P, Taborsky M, Kala P, et al. Left atrial appendage closure versus non-warfarin oral anticoagulation in atrial fibrillation: 4-year outcomes of PRAGUE-17. J Am Coll Cardiol. 2021. - PubMed
-
- Korsholm K, Damgaard D, Valentin JB, Packer EJS, Odenstedt J, Sinisalo J, et al. Left atrial appendage occlusion vs novel oral anticoagulation for stroke prevention in atrial fibrillation: rationale and design of the multicenter randomized occlusion-AF trial. Am Heart J. 2021;243:28–38. doi: 10.1016/j.ahj.2021.08.020. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
