

Spatiotemporal spread of Plasmodium falciparum mutations for resistance to sulfadoxine-pyrimethamine across Africa, 1990-2020
- PMID: 35951528
- PMCID: PMC9371298
- DOI: 10.1371/journal.pcbi.1010317
Spatiotemporal spread of Plasmodium falciparum mutations for resistance to sulfadoxine-pyrimethamine across Africa, 1990-2020
Abstract
Background: Sulfadoxine-pyrimethamine (SP) is recommended in Africa in several antimalarial preventive regimens including Intermittent Preventive Treatment in pregnant women (IPTp), Intermittent Preventive Treatment in infants (IPTi) and Seasonal Malaria Chemoprevention (SMC). The effectiveness of SP-based preventive treatments are threatened in areas where Plasmodium falciparum resistance to SP is high. The prevalence of mutations in the dihydropteroate synthase gene (pfdhps) can be used to monitor SP effectiveness. IPTi-SP is recommended only in areas where the prevalence of the pfdhps540E mutation is below 50%. It has also been suggested that IPTp-SP does not have a protective effect in areas where the pfdhps581G mutation, exceeds 10%. However, pfdhps mutation prevalence data in Africa are extremely heterogenous and scattered, with data completely missing from many areas.
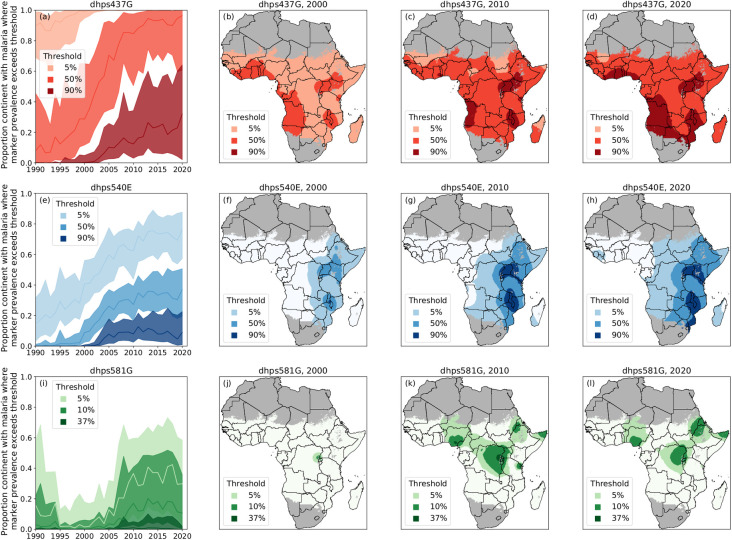
Methods and findings: The WWARN SP Molecular Surveyor database was designed to summarize dihydrofolate reductase (pfdhfr) and pfdhps gene mutation prevalence data. In this paper, pfdhps mutation prevalence data was used to generate continuous spatiotemporal surface maps of the estimated prevalence of the SP resistance markers pfdhps437G, pfdhps540E, and pfdhps581G in Africa from 1990 to 2020 using a geostatistical model, with a Bayesian inference framework to estimate uncertainty. The maps of estimated prevalence show an expansion of the pfdhps437G mutations across the entire continent over the last three decades. The pfdhps540E mutation emerged from limited foci in East Africa to currently exceeding 50% estimated prevalence in most of East and South East Africa. pfdhps540E distribution is expanding at low or moderate prevalence in central Africa and a predicted focus in West Africa. Although the pfdhps581G mutation spread from one focus in East Africa in 2000, to exceeding 10% estimated prevalence in several foci in 2010, the predicted distribution of the marker did not expand in 2020, however our analysis indicated high uncertainty in areas where pfdhps581G is present. Uncertainty was higher in spatial regions where the prevalence of a marker is intermediate or where prevalence is changing over time.
Conclusions: The WWARN SP Molecular Surveyor database and a set of continuous spatiotemporal surface maps were built to provide users with standardized, current information on resistance marker distribution and prevalence estimates. According to the maps, the high prevalence of pfdhps540E mutation was to date restricted to East and South East Africa, which is reassuring for continued use of IPTi and SMC in West Africa, but continuous monitoring is needed as the pfdhps540E distribution is expanding. Several foci where pfdhps581G prevalence exceeded 10% were identified. More data on the pfdhps581G distribution in these areas needs to be collected to guide IPTp-SP recommendations. Prevalence and uncertainty maps can be utilized together to strategically identify sites where increased surveillance can be most informative. This study combines a molecular marker database and predictive modelling to highlight areas of concern, which can be used to support decisions in public health, highlight knowledge gaps in certain regions, and guide future research.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures






References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
