

EHRA expert consensus statement on arrhythmic mitral valve prolapse and mitral annular disjunction complex in collaboration with the ESC Council on valvular heart disease and the European Association of Cardiovascular Imaging endorsed cby the Heart Rhythm Society, by the Asia Pacific Heart Rhythm Society, and by the Latin American Heart Rhythm Society
- PMID: 35951656
- PMCID: PMC11636573
- DOI: 10.1093/europace/euac125
EHRA expert consensus statement on arrhythmic mitral valve prolapse and mitral annular disjunction complex in collaboration with the ESC Council on valvular heart disease and the European Association of Cardiovascular Imaging endorsed cby the Heart Rhythm Society, by the Asia Pacific Heart Rhythm Society, and by the Latin American Heart Rhythm Society
Abstract
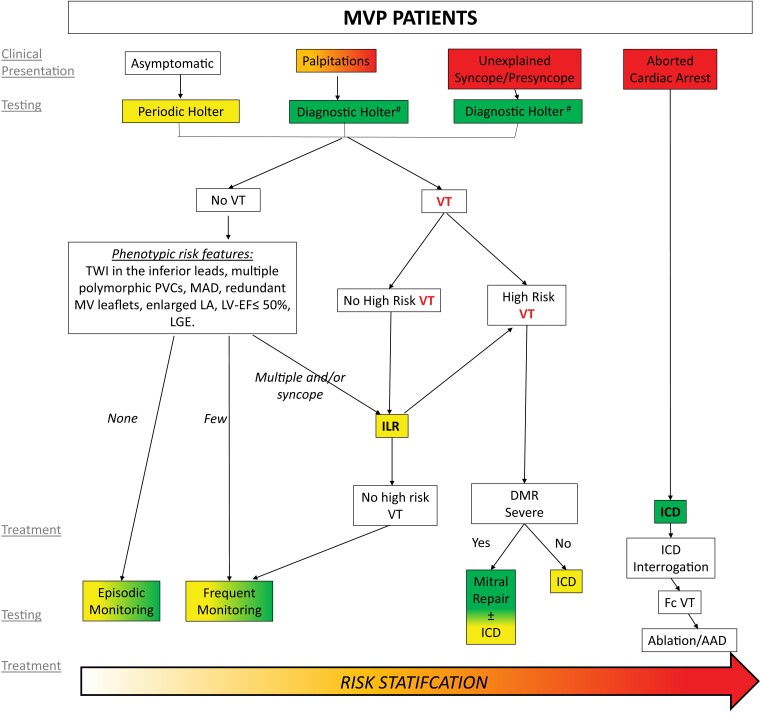
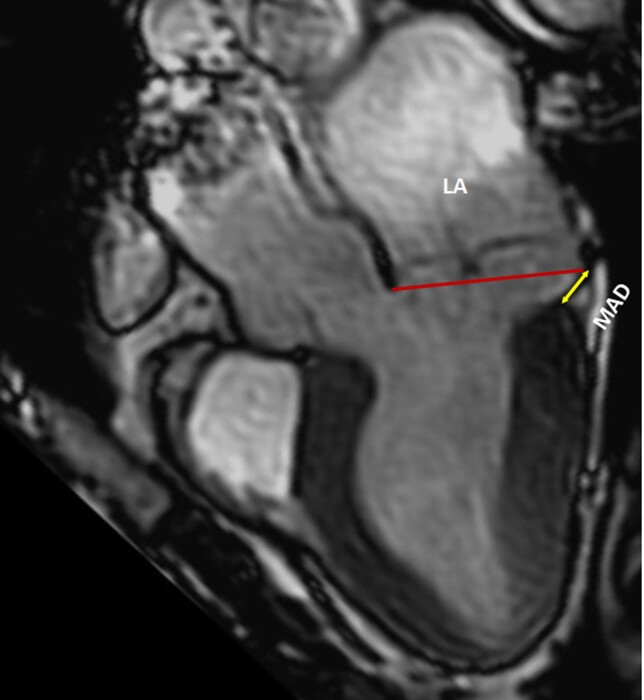
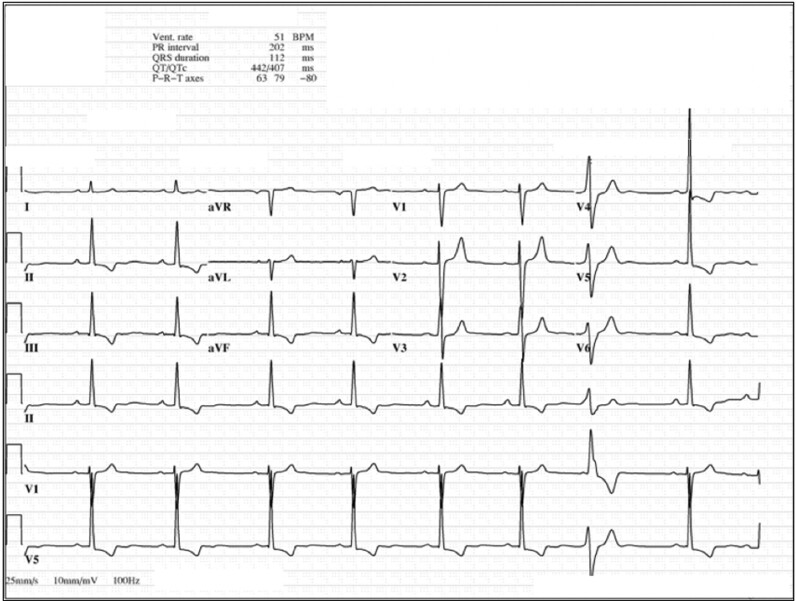
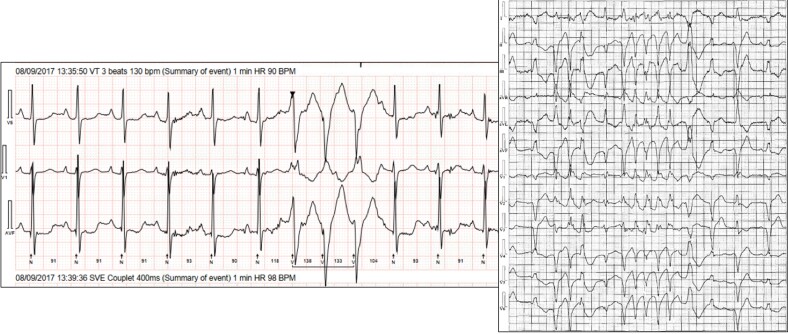
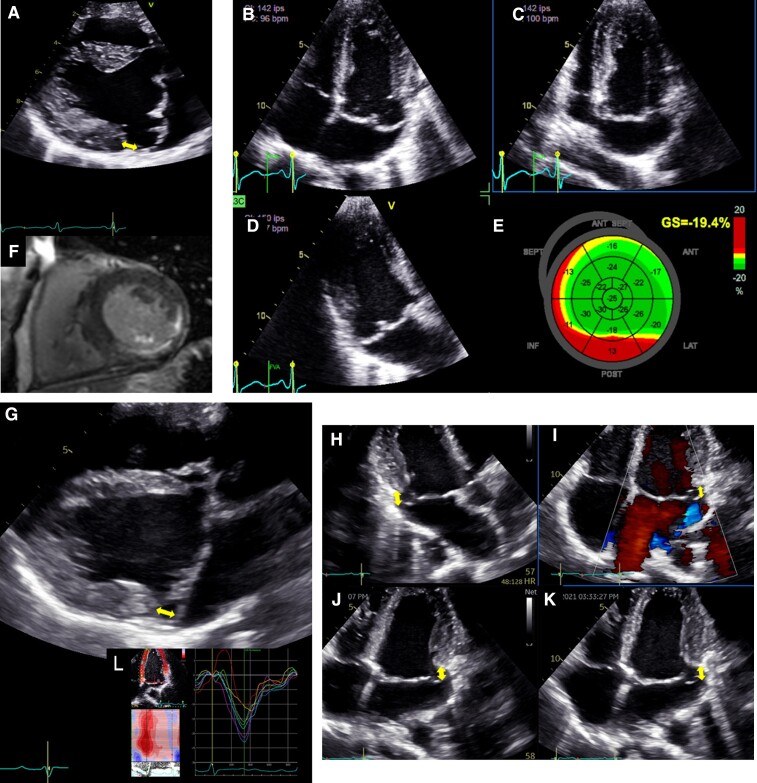
Risk stratification scheme. Risk stratification aiming at assessing the risk of VAs and SCD in patients with MVP, involving two phases based on the clinical and imaging context and the uncovered arrhythmia. In the absence of ventricular tachycardia, phenotypic risk features will trigger the intensity of screening for arrhythmia. Green boxes indicate green heart consensus statements and yellow boxes indicate yellow heart consensus statements. High risk - sustained VT, polymorphic NSVT, fast (>180 bpm) NSVT, VT/NSVT resulting in syncope. ICD = implantable cardioverter defibrillator; LA = left atrium; LGE = late gadolinium enhancement; LV-EF = left ventricular ejection fraction; MAD = mitral annular disjunction; MV = mitral valve; PVCs = premature ventricular contractions; TWI = T-wave inversion; VT = ventricular tachycardia. #Additional ECG monitoring method may be used such as loop recorders.
Keywords: Mitral annular disjunction; Mitral valve prolapse; Risk stratification; Sudden cardiac death; Ventricular arrhythmia.
Conflict of interest statement
Conflicts of interest: The authors have provided declaration of interest information for all relationships that might be perceived as real or potential sources of conflicts of interest. The full disclosures can be viewed in the Supplementary material online for this article, available online at [URL].
Figures
Comment in
-
Arrhythmic risk assessment of mitral valve prolapse pre- and post-mitral surgery-Authors' reply.Europace. 2023 Feb 16;25(2):778-779. doi: 10.1093/europace/euac209. Europace. 2023. PMID: 36413621 Free PMC article. No abstract available.
-
New-onset ventricular arrhythmias after surgery for mitral valve prolapse: how to classify and manage?Europace. 2023 Feb 16;25(2):776-777. doi: 10.1093/europace/euac207. Europace. 2023. PMID: 36413623 Free PMC article. No abstract available.
References
-
- Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet 2006;368:1005–11. - PubMed
-
- Freed LA, Levy D, Levine RA, Larson MG, Evans JC, Fuller DL, et al. Prevalence and clinical outcome of mitral-valve prolapse. N Engl J Med 1999;341:1–7. - PubMed
-
- Flack JM, Kvasnicka JH, Gardin JM, Gidding SS, Manolio TA, Jacobs DR Jr. Anthropometric and physiologic correlates of mitral valve prolapse in a biethnic cohort of young adults: the CARDIA study. Am Heart J 1999;138:486–92. - PubMed
-
- Theal M, Sleik K, Anand S, Yi Q, Yusuf S, Lonn E. Prevalence of mitral valve prolapse in ethnic groups. Can J Cardiol 2004;20:511–5. - PubMed
-
- Levine RA, Triulzi MO, Harrigan P, Weyman AE. The relationship of mitral annular shape to the diagnosis of mitral valve prolapse. Circulation 1987;75:756–67. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
