

Phenotypes of disease severity in a cohort of hospitalized COVID-19 patients: Results from the IMPACC study
- PMID: 35952496
- PMCID: PMC9359694
- DOI: 10.1016/j.ebiom.2022.104208
Phenotypes of disease severity in a cohort of hospitalized COVID-19 patients: Results from the IMPACC study
Erratum in
-
Corrigendum to "Phenotypes of disease severity in a cohort of hospitalized COVID-19 patients: results from the IMPACC study" [eBioMedicine 83 (2022) 104208].EBioMedicine. 2023 Dec;98:104860. doi: 10.1016/j.ebiom.2023.104860. Epub 2023 Nov 1. EBioMedicine. 2023. PMID: 37918220 Free PMC article. No abstract available.
Abstract
Background: Better understanding of the association between characteristics of patients hospitalized with coronavirus disease 2019 (COVID-19) and outcome is needed to further improve upon patient management.
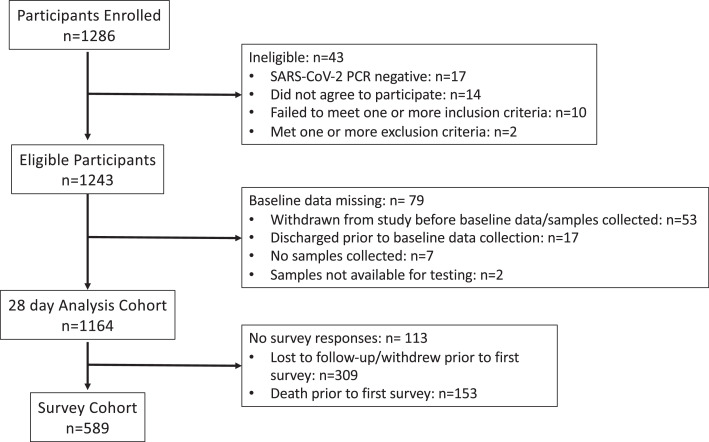
Methods: Immunophenotyping Assessment in a COVID-19 Cohort (IMPACC) is a prospective, observational study of 1164 patients from 20 hospitals across the United States. Disease severity was assessed using a 7-point ordinal scale based on degree of respiratory illness. Patients were prospectively surveyed for 1 year after discharge for post-acute sequalae of COVID-19 (PASC) through quarterly surveys. Demographics, comorbidities, radiographic findings, clinical laboratory values, SARS-CoV-2 PCR and serology were captured over a 28-day period. Multivariable logistic regression was performed.
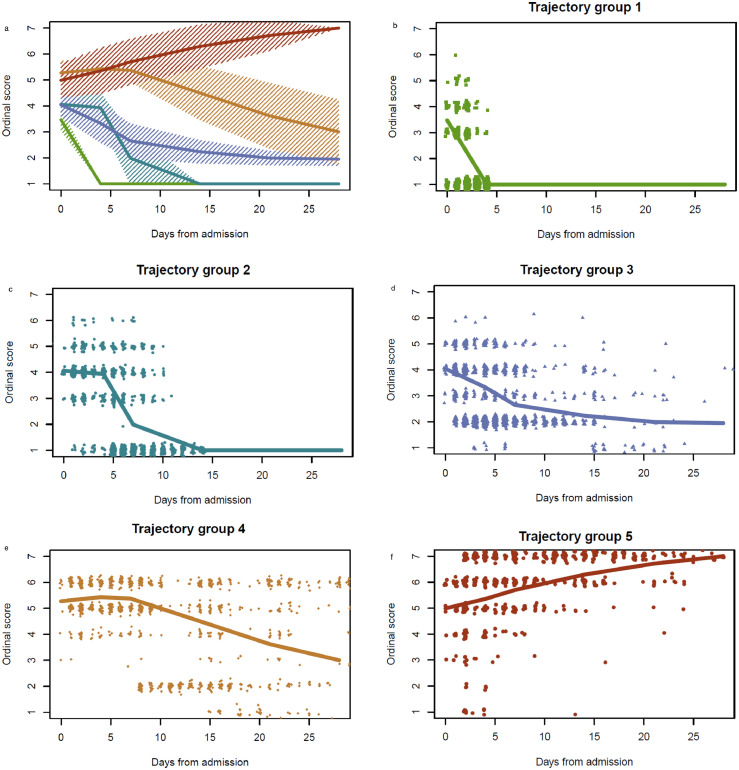
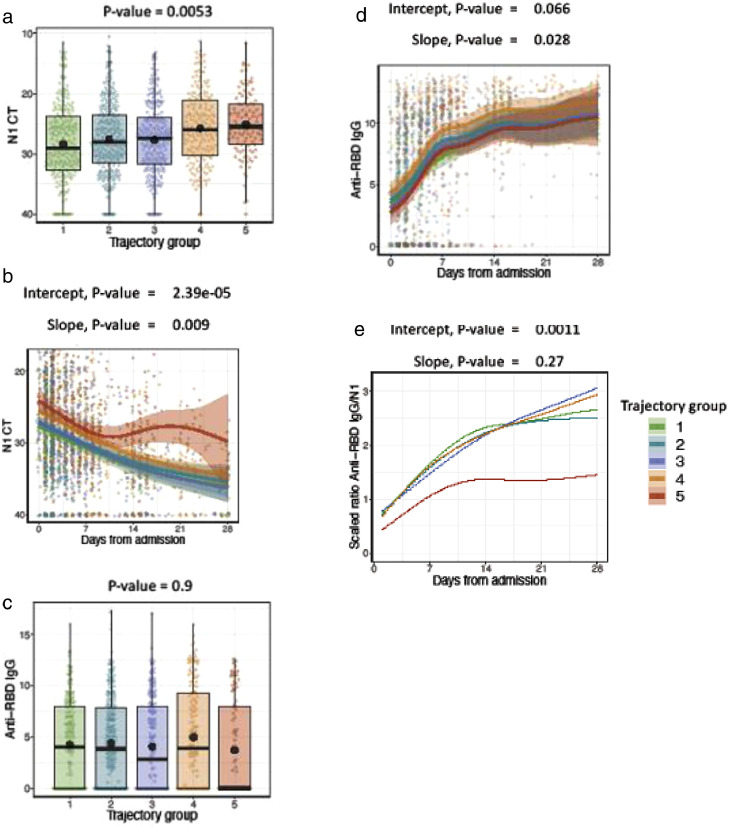
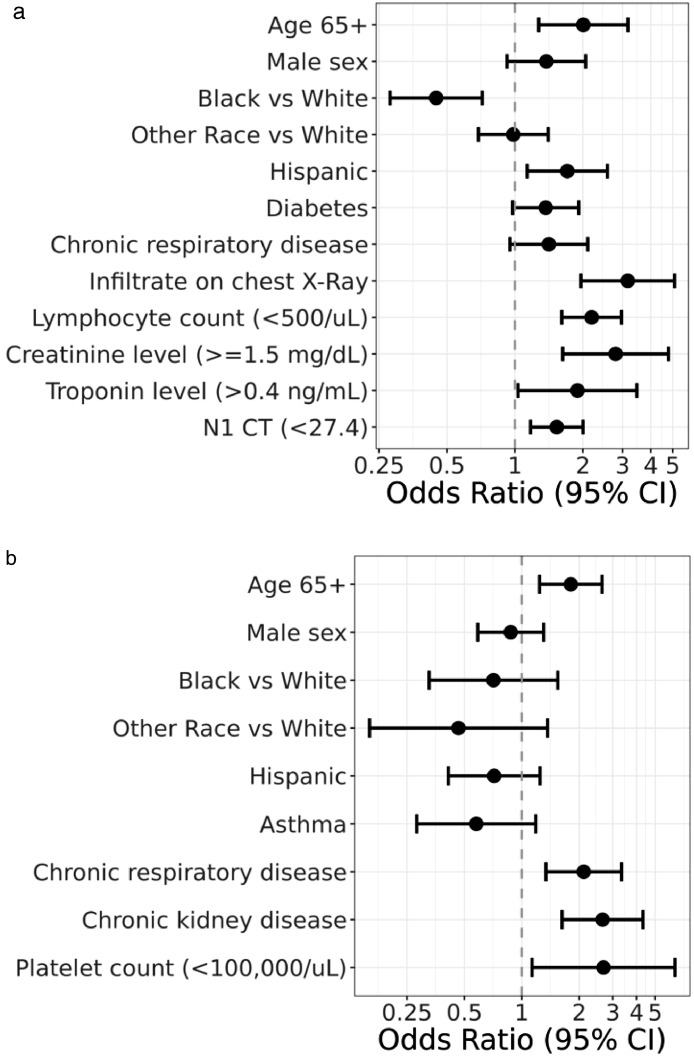
Findings: The median age was 59 years (interquartile range [IQR] 20); 711 (61%) were men; overall mortality was 14%, and 228 (20%) required invasive mechanical ventilation. Unsupervised clustering of ordinal score over time revealed distinct disease course trajectories. Risk factors associated with prolonged hospitalization or death by day 28 included age ≥ 65 years (odds ratio [OR], 2.01; 95% CI 1.28-3.17), Hispanic ethnicity (OR, 1.71; 95% CI 1.13-2.57), elevated baseline creatinine (OR 2.80; 95% CI 1.63- 4.80) or troponin (OR 1.89; 95% 1.03-3.47), baseline lymphopenia (OR 2.19; 95% CI 1.61-2.97), presence of infiltrate by chest imaging (OR 3.16; 95% CI 1.96-5.10), and high SARS-CoV2 viral load (OR 1.53; 95% CI 1.17-2.00). Fatal cases had the lowest ratio of SARS-CoV-2 antibody to viral load levels compared to other trajectories over time (p=0.001). 589 survivors (51%) completed at least one survey at follow-up with 305 (52%) having at least one symptom consistent with PASC, most commonly dyspnea (56% among symptomatic patients). Female sex was the only associated risk factor for PASC.
Interpretation: Integration of PCR cycle threshold, and antibody values with demographics, comorbidities, and laboratory/radiographic findings identified risk factors for 28-day outcome severity, though only female sex was associated with PASC. Longitudinal clinical phenotyping offers important insights, and provides a framework for immunophenotyping for acute and long COVID-19.
Funding: NIH.
Keywords: Antibody; COVID-19; SARS-CoV-2; Viral load.
Copyright © 2022 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests J.S reports funds paid to institution by the National Institute of Health - National Institute of Allergy and Infectious Diseases for the completion of this manuscript. C.S.C reports funds from NHLBI, has grants/contracts from Bayer, Roche-Genentech, Quantum Leap Healthcare Collaborative and received consulting fees from Vasomune, Gen1e Life Sciences, Cellenkos, Janssen. C.B.C reports funds paid to institution from the National Institute of Health - National Institute of Allergy and Infectious Diseases for the completion of this manuscript. C.B.C also reports a grant paid to institution by the Bill & Melinda Gates Foundation for Covid-19 work. C.B.C is a consultant for bioMerieux on clinical biomarkers. He reports his participation on a data safety monitoring board or advisory board for the Convalescent plasma Covid-19 study for the National Heart, Lung and Blood Institute (NHLBI). CBC is also President, Board of Directors for the National Foundation of Emergency Medicine (NFEM), a non-profit supporting emergency medicine research and researchers. M.K reports funds paid to institution for grants or contracts from the National Institute of Health. L.B reports grant awarded to institution from the National Institute of Health - National Institute of Allergy and Infectious Diseases. A.C.S reports funds paid to institution by the National Institute of Health for the completion of this manuscript (NIH U19 AI089992 – NIH K24 AG042489). F.KR has received funds from the National Institute of Allergy and Infectious Diseases Collaborative Influenza Vaccine Innovation Centers (CIVIC) contract 75N93019C00051, the National Institute of Health - Centers of Excellence for influenza Research and Response, (CEIRR), 75N93021C00014, the JPB Foundation and the Open Philanthropy Project (research grant 2020-215611, 5384), the National Cancer Institute, National Institutes of Health, under Contract No. 75N91019D00024, Task Order No. 75N91020F00003 and Research funding from Pfizer for development of animal models for SARS-CoV-2. F.KR receives royalties from Avimex, and receives consulting fees from Pfizer, Seqirus, Avimex and Third Rock Ventures. F.KR has received several payments or honoraria for academic lectures over the past two years. F. KR is listed as a co-inventor on patents filed for applications relating to SARS-CoV-2 serological assays (the “Serology Assays”) and NDV-based SARS-CoV-2 vaccines. H.vB reports receipt of the following grants paid to institution: National Institute of Health Centers of Excellence for influenza Research and Response, (CEIRR - 75N93021C00014), and National Institute of Health (Dengue Human Immunology Project Consortium - Mount Sinai IMPACC COVID-19 Cores - U19 AI118610 S1). D. E reports funds paid to institution for grants or contracts from the National Institute of Health. D.E is a statistician on the Data Safety Monitoring Board for the COLSTAT Trial. D.E is on the board of Directors for the Society for Clinical Trials. V.S is listed as a co-inventor on a patent filed relating to SARS-CoV-2 serological assays (the “Serology Assays”). R.M reports a grant from the National Institute of Health for the completion of this manuscript (AI 089992). R. M served as a Counselor for the Society of Leukocyte Biology from 2018 to 2021. S.K is a personal consultant related to ImmPort data repository for Peraton. O.L reports funds paid to institution by the National Institute of Health - National Institute of Allergy and Infectious Diseases for the completion of this manuscript (1-U19-AI118608-01A1). O.L received payments in the past 36 months from Midsized Bank Coalition of America (MBCA) and Moody's Analytics for presentations regarding the coronavirus pandemic. D.J.E reports funds paid to institution for grants or contracts from the National Institute of Health. K.C.N reports having received grants paid to institution from the following institutes in the past 36 months: National Institute of Allergy and Infectious Diseases (NIAID), National Heart, Lung, and Blood Institute (NHLBI), National Institute of Environmental Health Sciences (NIEHS), and Food Allergy Research & Education (FARE). K.C.N receives consulting fees from Excellergy, Eli Lilly, Red Tree Ventures, and Phylaxis. K.C.N has one Licensee: Alladapt and Before Brands (Application number: US15/048,609) for Mixed allergen composition and methods for using the same. K.C.N has two patents issued: Granulocyte-based methods for detecting and monitoring immune system disorders (Application number: US12/686,121), and Methods and Assays for Detecting and Quantifying Pure Subpopulations of White Blood Cells in Immune System Disorders (Application number: US12/610,94). K.C.N is the director of the World Allergy Organization Center of Excellence for Stanford and a co-founder of Seed Health, IgGenix, ClostraBio, and ImmuneID. K.C.N is also a co-founder of Before Brands, Alladapt, and Latitude and an advisor for Cour Pharma. K.C.N is a member of the national scientific committee for the Immune Tolerance Network (ITN) and the National Institutes of Health (NIH) clinical research centers. C.L.H reports a grant awarded to institution by the National Institute of Health and the American Lung Association. C.L.H also reports having received consulting fees from the National Institute of Health. C.L.H has received payment for medical grand rounds at institution and support for attending meetings and/or travel from Critical care trialists, critical care reviews and multiple universities. C.L.H is on the data safety monitoring board of QuantumHealth for iSPY COVID and is on the board of directors for the American Thoracic Society. W.M reports a grant from the National Institute of Health – National Institute of Allergy and Infectious Diseases for the completion of this manuscript (NIH NIAID R01AI14583). J.P.M reports funds paid to institution for grants or contracts from the National Institute of Health for the completion of this manuscript (NIH Grant # 3U19AI062629-17S2). M.A.A reports a grant from the National Institute of Health - National Institute of Allergy and Infectious Diseases for the completion of this manuscript (5U54AI142766-03). L.E reports grant awarded to institution from the National Institute of Health (NIH R01AI104870-S1). E.M reports funds paid to institution for grants or contracts from the National Institute of Health for the completion of this manuscript (NIH R01 AI104870S1). E.M also reports having received the following grants paid to institution in the past 36 months: the Babson Diagnostics Grant, the Austin Public Health Grant, and K08 26-1616-11. E.M received payments for lectures for the MS Association of America. E. M received payments for the participation in the advisory boards of Genentech, Horizon, Teva and Viela Bio. G.M receives consulting fees from Gilead. B.PE reports a grant from the National Institute of Health - National Institute of Allergy and Infectious Diseases for the completion of this manuscript. E.F.R reports funds paid to institution by the National Institute of Health - National Institute of Allergy and Infectious Diseases for the completion of this manuscript (NIAID U19AI12891303). M.C.A reports funds received from the National Institute of Health for the completion of this manuscript (NIH – R01AI32774) and funding by the National Institute of Allergy and Infectious Diseases for travel to present data related to this study. P.M.B is a federal employee serving as project scientist for this project but has no role in funding decisions or oversight for relevant grants. N.R reports funds paid to institution by the National Institute of Health - National Institute of Allergy and Infectious Diseases for the completion of this manuscript. N.R reports contracts with Lilly and Sanofi for conduct of Covid-19 clinical trials. N.R receives consulting fees from ICON EMMES for consulting on safety for Covid-19 clinical trials. N.R is an associate editor for Clinical infectious diseases. The remaining authors declare that they have no conflict of interest.
Figures
References
-
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. - PubMed
-
- World health organization. WHO R&D blueprint novel coronavirus COVID-19 therapeutic trial synopsis. 2020.https://www.who.int/blueprint/priority-diseases/key-action/COVID-19_Trea.... Accessed 18 February 2020.
-
- Centers for Disease Control and Prevention. Research use only 2019-novel coronavirus (2019-nCoV) real-time RT-PCR primers and probes. 2020, June 6. https://www.cdc.gov/coronavirus/2019-ncov/lab/rt-pcr-panel-primer-probes....
Publication types
MeSH terms
Substances
Grants and funding
- U19 AI090023/AI/NIAID NIH HHS/United States
- U19 AI057229/AI/NIAID NIH HHS/United States
- S10 OD026880/OD/NIH HHS/United States
- U19 AI062629/AI/NIAID NIH HHS/United States
- U19 AI077439/AI/NIAID NIH HHS/United States
- U19 AI128910/AI/NIAID NIH HHS/United States
- R01 AI104870/AI/NIAID NIH HHS/United States
- U19 AI118626/AI/NIAID NIH HHS/United States
- U19 AI167891/AI/NIAID NIH HHS/United States
- U19 AI167903/AI/NIAID NIH HHS/United States
- U19 AI125357/AI/NIAID NIH HHS/United States
- R01 AI145835/AI/NIAID NIH HHS/United States
- I01 BX005023/BX/BLRD VA/United States
- U19 AI128913/AI/NIAID NIH HHS/United States
- R01 AI132774/AI/NIAID NIH HHS/United States
- U19 AI118608/AI/NIAID NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- U54 AI142766/AI/NIAID NIH HHS/United States
- U19 AI057266/AI/NIAID NIH HHS/United States
- K08 AA027837/AA/NIAAA NIH HHS/United States
- U19 AI118610/AI/NIAID NIH HHS/United States
- K08 HL141623/HL/NHLBI NIH HHS/United States
- P01 AI153559/AI/NIAID NIH HHS/United States
- S10 OD030463/OD/NIH HHS/United States
- R01 AI135803/AI/NIAID NIH HHS/United States
- U19 AI089992/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
