

Clinical presentation and virological assessment of confirmed human monkeypox virus cases in Spain: a prospective observational cohort study
- PMID: 35952705
- PMCID: PMC9533900
- DOI: 10.1016/S0140-6736(22)01436-2
Clinical presentation and virological assessment of confirmed human monkeypox virus cases in Spain: a prospective observational cohort study
Erratum in
-
Department of Error.Lancet. 2022 Dec 10;400(10368):2048. doi: 10.1016/S0140-6736(22)02504-1. Lancet. 2022. PMID: 36502841 Free PMC article. No abstract available.
Abstract
Background: In May, 2022, several European countries reported autochthonous cases of monkeypox, which rapidly spread globally. Early reports suggest atypical presentations. We aimed to investigate clinical and virological characteristics of cases of human monkeypox in Spain.
Methods: This multicentre, prospective, observational cohort study was done in three sexual health clinics in Madrid and Barcelona, Spain. We enrolled all consecutive patients with laboratory-confirmed monkeypox from May 11 to June 29, 2022. Participants were offered lesion, anal, and oropharynx swabs for PCR testing. Participant data were collected by means of interviews conducted by dermatologists or specialists in sexually transmitted infections and were recorded using a standard case report form. Outcomes assessed in all participants with a confirmed diagnosis were demographics, smallpox vaccination, HIV status, exposure to someone with monkeypox, travel, mass gathering attendance, risk factors for sexually transmitted infections, sexual behaviour, signs and symptoms on first presentation, virological results at multiple body sites, co-infection with other sexually transmitted pathogens, and clinical outcomes 14 days after the initial presentation. Clinical outcomes were followed up until July 13, 2022.
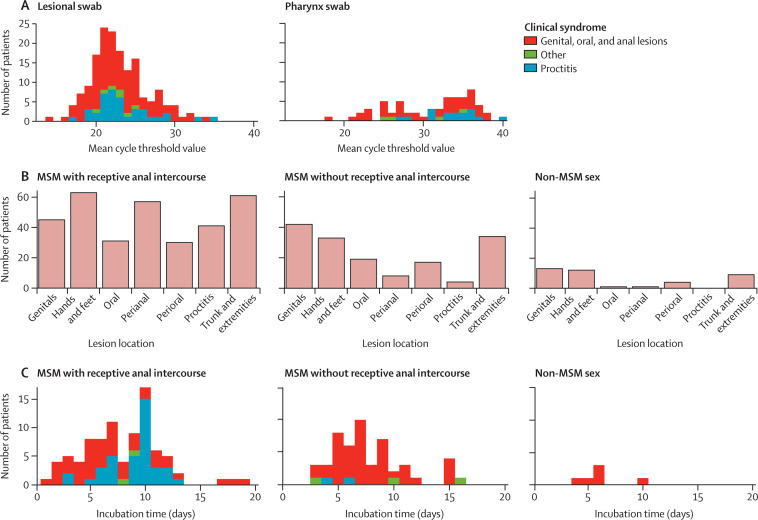
Findings: 181 patients had a confirmed monkeypox diagnosis and were enrolled in the study. 166 (92%) identified as gay men, bisexual men, or other men who have sex with men (MSM) and 15 (8%) identified as heterosexual men or heterosexual women. Median age was 37·0 years (IQR 31·0-42·0). 32 (18%) patients reported previous smallpox vaccination, 72 (40%) were HIV-positive, eight (11%) had a CD4 cell count less than 500 cells per μL, and 31 (17%) were diagnosed with a concurrent sexually transmitted infection. Median incubation was 7·0 days (IQR 5·0-10·0). All participants presented with skin lesions; 141 (78%) participants had lesions in the anogenital region, and 78 (43%) in the oral and perioral region. 70 (39%) participants had complications requiring treatment: 45 (25%) had a proctitis, 19 (10%) had tonsillitis, 15 (8%) had penile oedema, six (3%) an abscess, and eight (4%) had an exanthem. Three (2%) patients required hospital admission. 178 (99%) of 180 swabs from skin lesions collected tested positive, as did 82 (70%) of 117 throat swabs. Viral load was higher in lesion swabs than in pharyngeal specimens (mean cycle threshold value 23 [SD 4] vs 32 [6], absolute difference 9 [95% CI 8-10]; p<0·0001). 108 (65%) of 166 MSM reported anal-receptive sex. MSM who engaged in anal-receptive sex presented with proctitis (41 [38%] of 108 vs four [7%] of 58, absolute difference 31% [95% CI 19-44]; p<0·0001) and systemic symptoms before the rash (67 [62%] vs 16 [28%], absolute difference 34% [28-62]; p<0·0001) more frequently than MSM who did not engage in anal-receptive sex. 18 (95%) of 19 participants with tonsillitis reported practising oral-receptive sex. The median time from onset of lesions to formation of a dry crust was 10 days (IQR 7-13).
Interpretation: In our cohort, monkeypox caused genital, perianal, and oral lesions and complications including proctitis and tonsillitis. Because of the variability of presentations, clinicians should have a low threshold for suspicion of monkeypox. Lesion swabs showed the highest viral loads, which, combined with the history of sexual exposure and the distribution of lesions, suggests close contact is probably the dominant transmission route in the current outbreak.
Funding: None.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures

Comment in
-
How does monkeypox spread? What scientists know.Nature. 2022 Aug;608(7924):655-656. doi: 10.1038/d41586-022-02178-w. Nature. 2022. PMID: 35953575 No abstract available.
-
In monkeypox, risk for some symptoms was greater in MSM with vs. without receptive anal contact.Ann Intern Med. 2022 Dec;175(12):JC142. doi: 10.7326/J22-0092. Epub 2022 Dec 6. Ann Intern Med. 2022. PMID: 36469917
References
-
- UK Health Security Agency Investigation into monkeypox outbreak in England: technical briefing 1. 2022. https://www.gov.uk/government/publications/monkeypox-outbreak-technical-...
-
- WHO Multi-country monkeypox outbreak in non-endemic countries: update. 2022. https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON388#:...
-
- European Centre for Disease Prevention and Control Epidemiological update: monkeypox multi-country outbreak. 2022. https://www.ecdc.europa.eu/en/news-events/epidemiological-update-monkeyp...
-
- Damon IK. In: Fields virology. Knipe DM, Howley PM, editors. Lippincott Williams & Wilkins, a Wolters Kluwer business; Philadephia, PA: 2013. Poxviruses; pp. 2160–2184.
-
- Dixon CW. J & A Churchill; London: 1962. Smallpox.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
