

Persistence, adherence, healthcare resource utilization and costs for ocrelizumab in the real-world of the Campania Region of Italy
- PMID: 35953597
- PMCID: PMC9618479
- DOI: 10.1007/s00415-022-11320-7
Persistence, adherence, healthcare resource utilization and costs for ocrelizumab in the real-world of the Campania Region of Italy
Abstract
Aims: We aim to provide real-world evidence on the use of ocrelizumab for treating multiple sclerosis (MS), with specific regard to prescription pattern, adherence, persistence, healthcare resource utilization and related costs, also in relation to other disease-modifying treatments (DMTs).
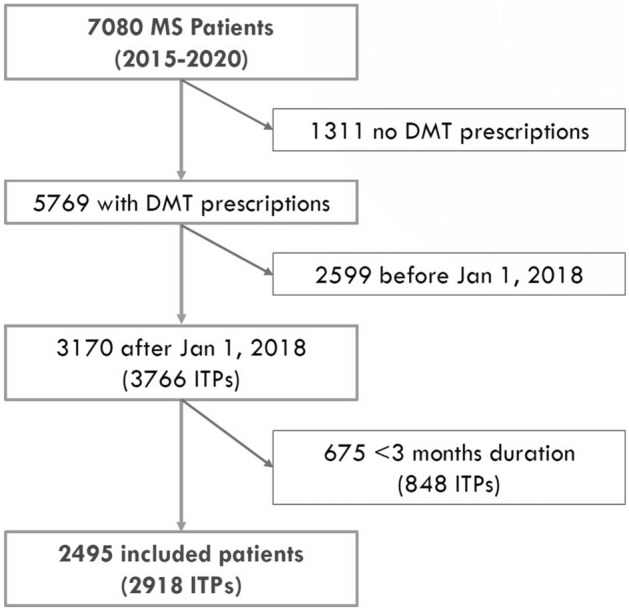
Methods: We included 2495 people with MS from the Campania Region (South Italy) who received first or switch DMT prescription from Jan 2018 to Dec 2020, and with at least 6-month follow-up. We collected hospital discharge records, drug prescriptions, and related costs, and calculated persistence (time from first prescription to discontinuation or switch to other DMT), adherence (proportion of days covered (PDC)), annualized hospitalization rate (AHR) for MS-related hospital admissions, and DMT costs.
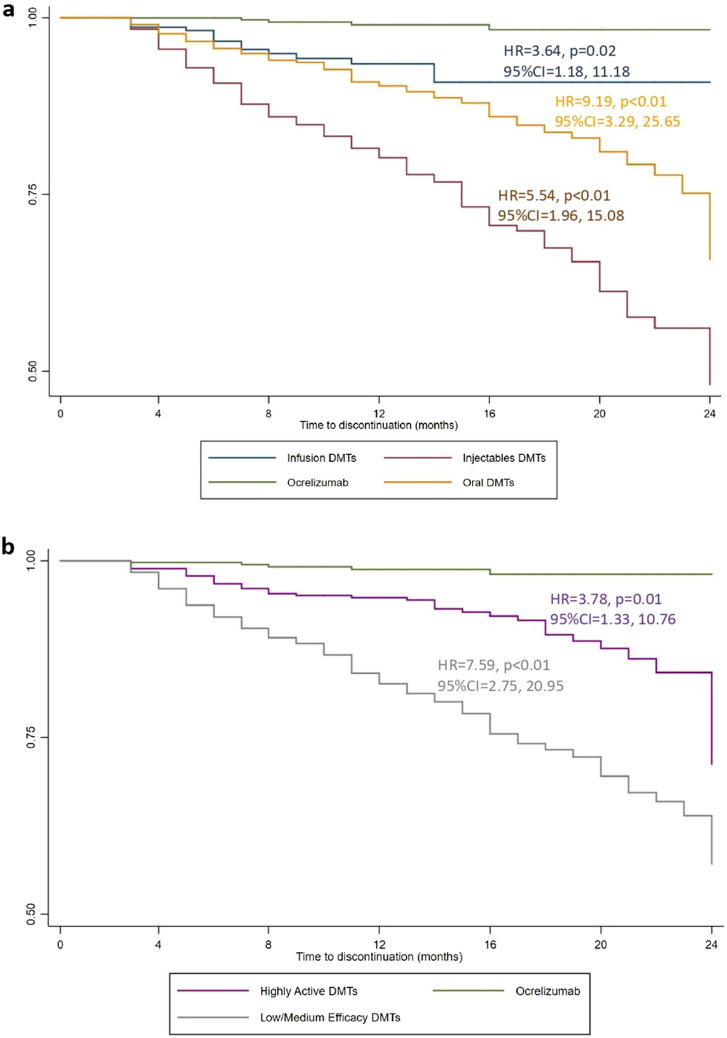
Results: Ocrelizumab was the most commonly prescribed DMT (n = 399; age = 45.74 ± 10.98 years; females = 224), after dimethyl fumarate (n = 588) and fingolimod (n = 401); 26% patients treated with ocrelizumab were naïve. When compared with ocrelizumab, the risk of discontinuation was higher for other highly active DMTs (HR = 3.78; p = 0.01), and low/medium efficacy DMTs (HR = 7.59; p < 0.01). When compared with ocrelizumab, PDC was similar to other highly active DMTs (Coeff = 0.01; p = 0.31), but higher for low/medium efficacy DMTs (Coeff = 0.09; p < 0.01). When compared with ocrelizumab, AHR was similar to other highly active DMTs (Coeff = 0.01; p = 0.51), and low/medium efficacy DMTs (Coeff = 0.01; p = 0.55). When compared with ocrelizumab, DMT monthly costs were higher for other highly active DMTs (Coeff = 92.30; p < 0.01), but lower for low/medium efficacy DMTs (Coeff = - 1043.61; p < 0.01).
Discussion: Ocrelizumab was among the most frequently prescribed DMTs, with 26% prescriptions to treatment-naïve patients, suggesting its relevance in addressing unmet clinical needs (e.g., first approved treatment for primary progressive MS). Ocrelizumab was associated with the highest persistence, confirming its favorable benefit-risk profile. Costs for ocrelizumab were lower than those associated to similarly effective DMTs, in absence of changes in healthcare resource utilization.
Keywords: Costs; Multiple sclerosis; Ocrelizumab; Persistence, adherence; Treatment.
© 2022. The Author(s).
Conflict of interest statement
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by Roche SpA, Monza, Italy, on the basis of a Sponsored Research Agreement. Marcello Moccia has received research grants from ECTRIMS-MAGNIMS, UK MS Society, and Merck; honoraria from Biogen, BMS Celgene, Merck, Roche, and Sanofi-Genzyme. Antonio Carotenuto has received research grants from Almirall, research grants from ECTRIMS-MAGNIMS and honoraria from Almirall, Biogen, Roche Sanofi-Genzyme and Novartis. Maria Petracca has received research grants from Italian MS Foundation and Baroni Foundation, honoraria from HEALTH&LIFE S.r.l. and Biogen and sponsorship for travel/meeting expenses from Novartis, Roche and Merck. Roberta Lanzillo has received honoraria from Merck, Novartis, Roche, Sanofi-Genzyme, and Teva. Vincenzo Brescia Morra has received research grants from the Italian MS Society, and Roche; and honoraria from Bayer, Biogen, Merck, Mylan, Novartis, Roche, Sanofi-Genzyme, and Teva. Other authors have nothing to disclose.
Figures
References
-
- Wolinsky JS, Arnold DL, Brochet B, et al. Long-term follow-up from the ORATORIO trial of ocrelizumab for primary progressive multiple sclerosis: a post-hoc analysis from the ongoing open-label extension of the randomised, placebo-controlled, phase 3 trial. Lancet Neurol. 2020;19:998–1009. doi: 10.1016/S1474-4422(20)30342-2. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
