

Ecological effects of selective oral decontamination on multidrug-resistance bacteria acquired in the intensive care unit: a case-control study over 5 years
- PMID: 35953676
- PMCID: PMC9463265
- DOI: 10.1007/s00134-022-06826-7
Ecological effects of selective oral decontamination on multidrug-resistance bacteria acquired in the intensive care unit: a case-control study over 5 years
Abstract
Purpose: This case-control study investigated the long-term evolution of multidrug-resistant bacteria (MDRB) over a 5-year period associated with the use of selective oropharyngeal decontamination (SOD) in the intensive care unit (ICU). In addition, effects on health care-associated infections and ICU mortality were analysed.
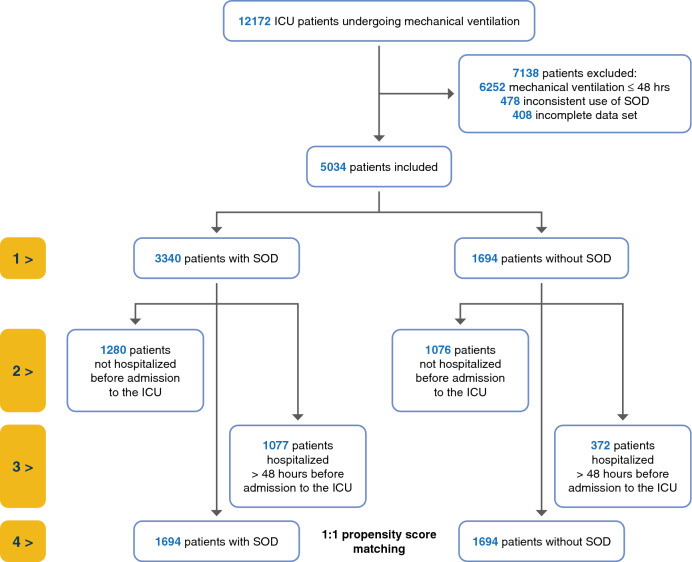
Methods: We investigated patients undergoing mechanical ventilation > 48 h in 11 adult ICUs located at 3 campuses of a university hospital. Administrative, clinical, and microbiological data which were routinely recorded electronically served as the basis. We analysed differences in the rates and incidence densities (ID, cases per 1000 patient-days) of MDRB associated with SOD use in all patients and stratified by patient origin (outpatient or inpatient). After propensity score matching, health-care infections and ICU mortality were compared.
Results: 5034 patients were eligible for the study. 1694 patients were not given SOD. There were no differences in the incidence density of MDRB when SOD was used, except for more vancomycin-resistant Enterococcus faecium (0.72/1000 days vs. 0.31/1000 days, p < 0.01), and fewer ESBL-producing Klebsiella pneumoniae (0.22/1000 days vs. 0.56/1000 days, p < 0.01). After propensity score matching, SOD was associated with lower incidence rates of ventilator-associated pneumonia and death in the ICU but not with ICU-acquired bacteremia or urinary tract infection.
Conclusions: Comparisons of the ICU-acquired MDRB over a 5-year period revealed no differences in incidence density, except for lower rate of ESBL-producing Klebsiella pneumoniae and higher rate of vancomycin-resistant Enterococcus faecium with SOD. Incidence rates of ventilator-associated pneumonia and death in the ICU were lower in patients receiving SOD.
Keywords: Klebsiella pneumoniae/drug effects; Methicillin-resistant Staphylococcus aureus/drug effects; Polymyxins/drug effects; Pseudomonas aeruginosa/drug effects; Selective oral decontamination, selective digestive decontamination, antimicrobial resistance, intensive care units/statistics and numerical data; Vancomycin/drug effects.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Comment in
-
Decontamination regimens: do not forget half of the protocol.Intensive Care Med. 2023 Jan;49(1):115-116. doi: 10.1007/s00134-022-06915-7. Epub 2022 Nov 9. Intensive Care Med. 2023. PMID: 36350353 No abstract available.
References
-
- de Smet AMGA, Kluytmans JAJW, Cooper BS, Mascini EM, Benus RFJ, van der Werf TS, van der Hoeven JG, Pickkers P, Bogaers-Hofman D, van der Meer NJM, Bernards AT, Kuijper EJ, Joore JCA, Leverstein-van Hall MA, Bindels AJGH, Jansz AR, Wesselink RMJ, de Jongh BM, Dennesen PJW, van Asselt GJ, te Velde LF, Frenay IHME, Kaasjager K, Bosch FH, van Iterson M, Thijsen SFT, Kluge GH, Pauw W, de Vries JW, Kaan JA, Arends JP, Aarts LPHJ, Sturm PDJ, Harinck HIJ, Voss A, Uijtendaal EV, Blok HEM, Thieme Groen ES, Pouw ME, Kalkman CJ, Bonten MJM. Decontamination of the digestive tract and oropharynx in ICU patients. N Engl J Med. 2009;360:20–31. doi: 10.1056/NEJMoa0800394. - DOI - PubMed
-
- Oostdijk EAN, Kesecioglu J, Schultz MJ, Visser CE, de Jonge E, van Essen EHR, Bernards AT, Purmer I, Brimicombe R, Bergmans D, van Tiel F, Bosch FH, Mascini E, van Griethuysen A, Bindels A, Jansz A, van Steveninck FAL, van der Zwet WC, Fijen JW, Thijsen S, de Jong R, Oudbier J, Raben A, van der Vorm E, Koeman M, Rothbarth P, Rijkeboer A, Gruteke P, Hart-Sweet H, Peerbooms P, Winsser LJ, van Elsacker-Niele AW, Demmendaal K, Brandenburg A, de Smet A, Bonten MJM. Effects of decontamination of the oropharynx and intestinal tract on antibiotic resistance in ICUs: a randomized clinical trial. JAMA. 2014;312:1429–1437. doi: 10.1001/jama.2014.7247. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
