

Immunotherapy for the Treatment of Squamous Cell Carcinoma: Potential Benefits and Challenges
- PMID: 35955666
- PMCID: PMC9368833
- DOI: 10.3390/ijms23158530
Immunotherapy for the Treatment of Squamous Cell Carcinoma: Potential Benefits and Challenges
Abstract
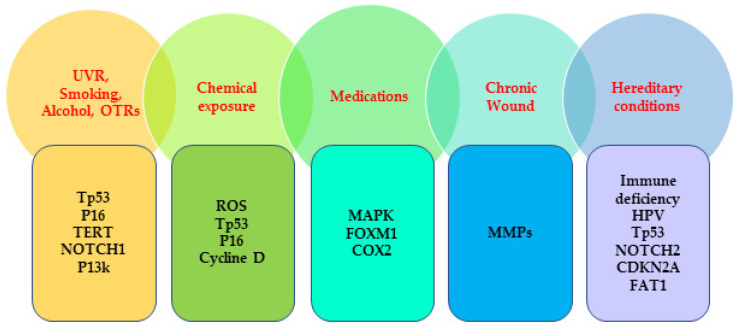
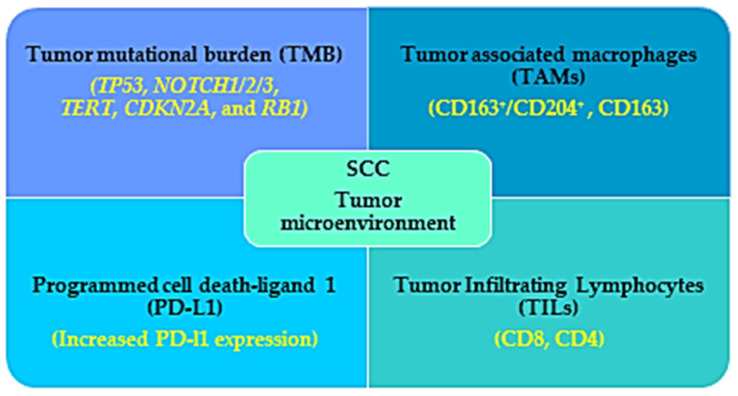
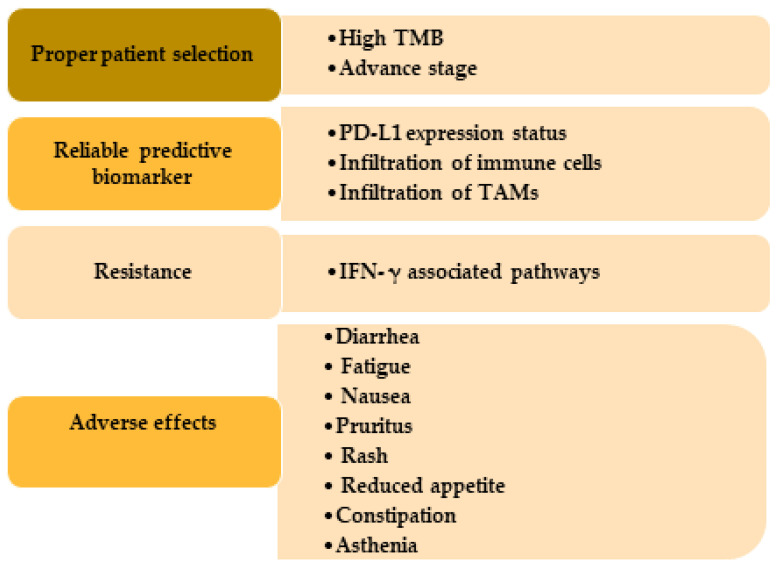
Melanoma and nonmelanoma skin cancers (NMSCs) are recognized as among the most common neoplasms, mostly in white people, with an increasing incidence rate. Among the NMSCs, squamous cell carcinoma (SCC) is the most prevalent malignancy known to affect people with a fair complexion who are exposed to extreme ultraviolet radiation (UVR), have a hereditary predisposition, or are immunosuppressed. There are several extrinsic and intrinsic determinants that contribute to the pathophysiology of the SCC. The therapeutic modalities depend on the SCC stages, from actinic keratosis to late-stage multiple metastases. Standard treatments include surgical excision, radiotherapy, and chemotherapy. As SCC represents a favorable tumor microenvironment with high tumor mutational burden, infiltration of immune cells, and expression of immune checkpoints, the SCC tumors are highly responsive to immunotherapies. Until now, there are three checkpoint inhibitors, cemiplimab, pembrolizumab, and nivolumab, that are approved for the treatment of advanced, recurrent, or metastatic SCC patients in the United States. Immunotherapy possesses significant therapeutic benefits for patients with metastatic or locally advanced tumors not eligible for surgery or radiotherapy to avoid the potential toxicity caused by the chemotherapies. Despite the high tolerability and efficiency, the existence of some challenges has been revealed such as, resistance to immunotherapy, less availability of the biomarkers, and difficulty in appropriate patient selection. This review aims to accumulate evidence regarding the genetic alterations related to SCC, the factors that contribute to the potential benefits of immunotherapy, and the challenges to follow this treatment regime.
Keywords: immunotherapy; nonmelanoma skin cancers (NMSCs); risk factors of SCC; squamous cell carcinoma (SCC).
Conflict of interest statement
The author declares no conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
