

Functional Precision Oncology: The Next Frontier to Improve Glioblastoma Outcome?
- PMID: 35955765
- PMCID: PMC9369403
- DOI: 10.3390/ijms23158637
Functional Precision Oncology: The Next Frontier to Improve Glioblastoma Outcome?
Abstract
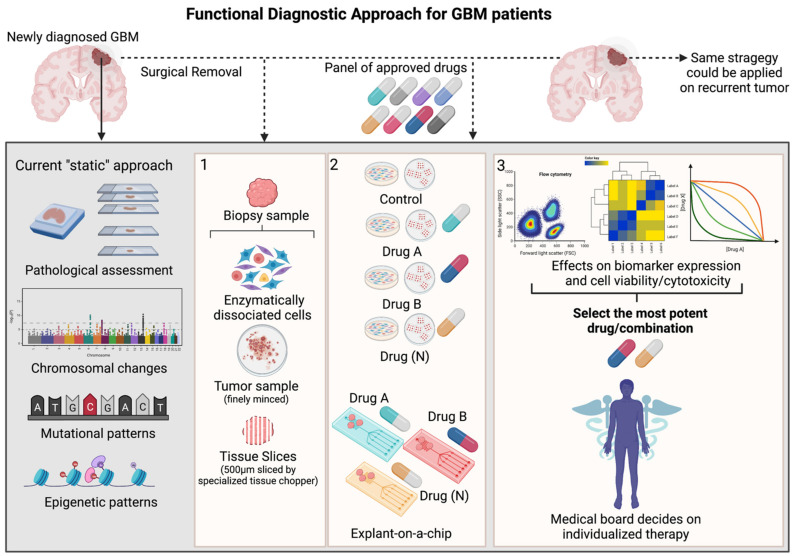
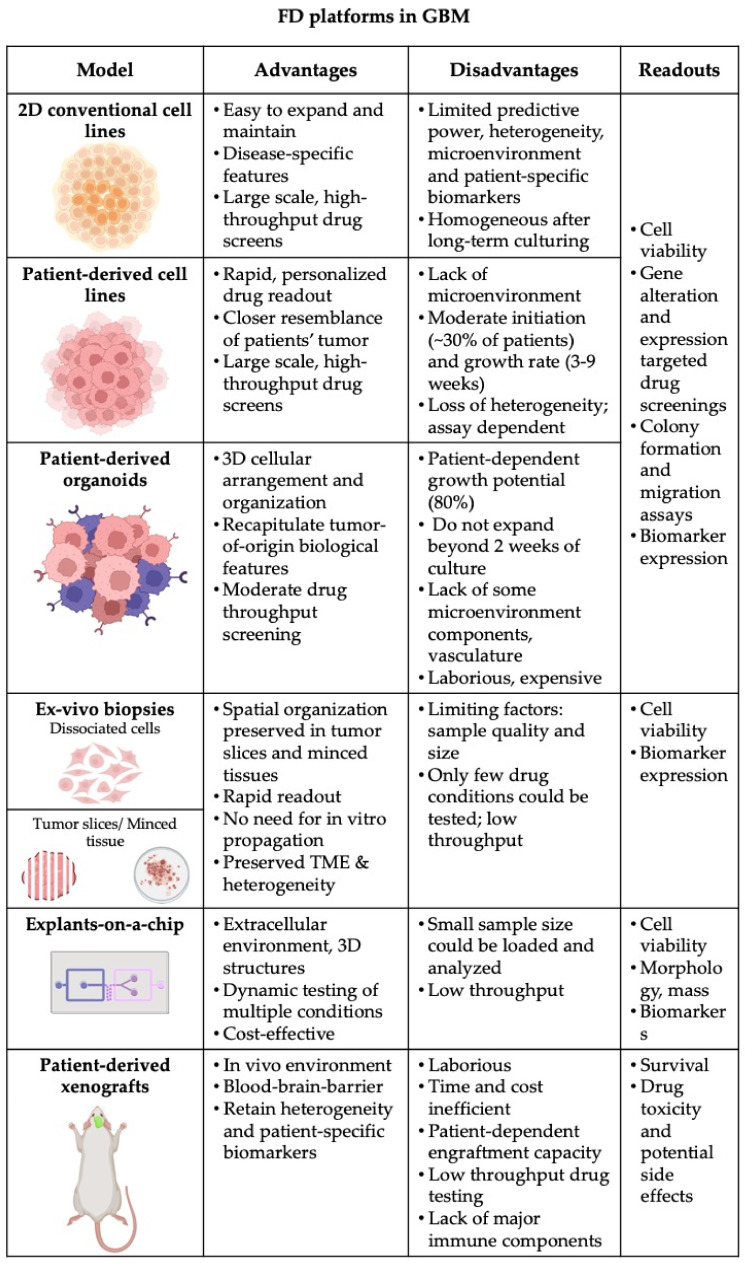
Glioblastoma remains the most malignant and intrinsically resistant brain tumour in adults. Despite intensive research over the past few decades, through which numerous potentially druggable targets have been identified, virtually all clinical trials of the past 20 years have failed to improve the outcome for the vast majority of GBM patients. The observation that small subgroups of patients displayed a therapeutic response across several unsuccessful clinical trials suggests that the GBM patient population probably consists of multiple subgroups that probably all require a distinct therapeutic approach. Due to extensive inter- and intratumoral heterogeneity, assigning the right therapy to each patient remains a major challenge. Classically, bulk genetic profiling would be used to identify suitable therapies, although the success of this approach remains limited due to tumor heterogeneity and the absence of direct relationships between mutations and therapy responses in GBM. An attractive novel strategy aims at implementing methods for functional precision oncology, which refers to the evaluation of treatment efficacies and vulnerabilities of (ex vivo) living tumor cells in a highly personalized way. Such approaches are currently being implemented for other cancer types by providing rapid, translatable information to guide patient-tailored therapeutic selections. In this review, we discuss the current state of the art of transforming technologies, tools and challenges for functional precision oncology and how these could improve therapy selection for GBM patients.
Keywords: drug sensitivity; functional precision oncology; glioblastoma.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Masui K., Gini B., Wykosky J., Zanca C., Mischel P.S., Furnari F.B., Cavenee W.K. A Tale of Two Approaches: Complementary Mechanisms of Cytotoxic and Targeted Therapy Resistance May Inform next-Generation Cancer Treatments. Carcinogenesis. 2013;34:725–738. doi: 10.1093/carcin/bgt086. - DOI - PMC - PubMed
-
- Sampaio M.M., Santos M.L.C., Marques H.S., Gonçalves V.L.d.S., Araújo G.R.L., Lopes L.W., Apolonio J.S., Silva C.S., Santos L.K.d.S., Cuzzuol B.R., et al. Chronic Myeloid Leukemia-from the Philadelphia Chromosome to Specific Target Drugs: A Literature Review. World J. Clin. Oncol. 2021;12:69–94. doi: 10.5306/wjco.v12.i2.69. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
