

MicroRNA in Acromegaly: Involvement in the Pathogenesis and in the Response to First-Generation Somatostatin Receptor Ligands
- PMID: 35955787
- PMCID: PMC9368811
- DOI: 10.3390/ijms23158653
MicroRNA in Acromegaly: Involvement in the Pathogenesis and in the Response to First-Generation Somatostatin Receptor Ligands
Abstract
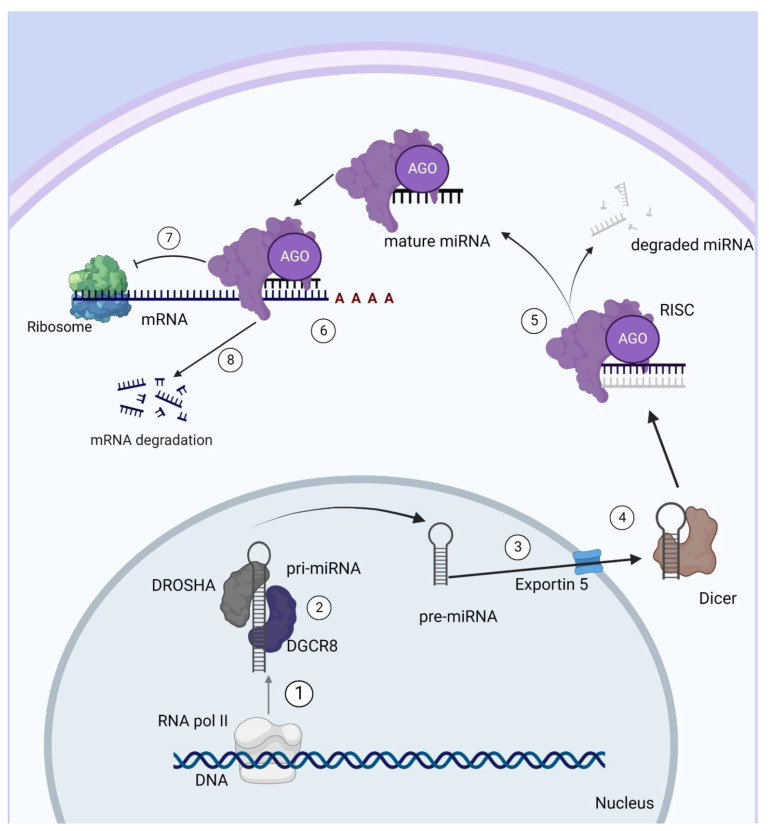
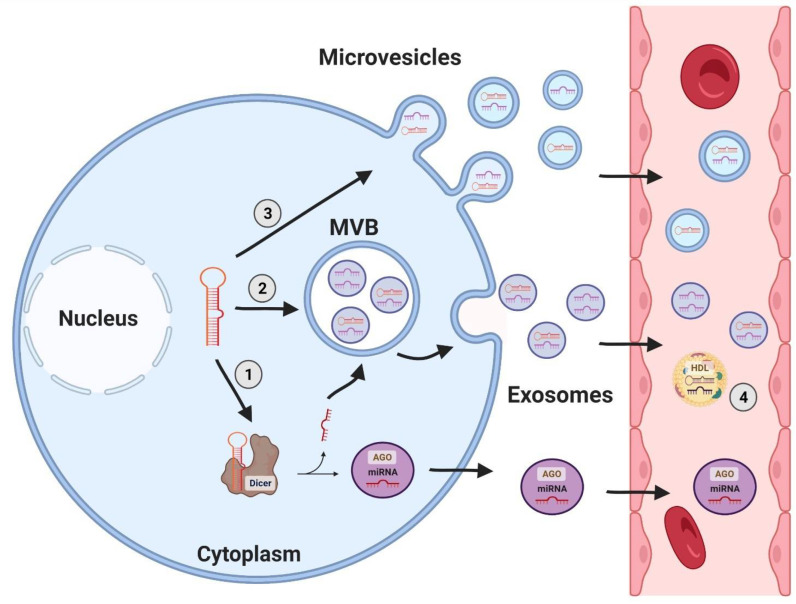
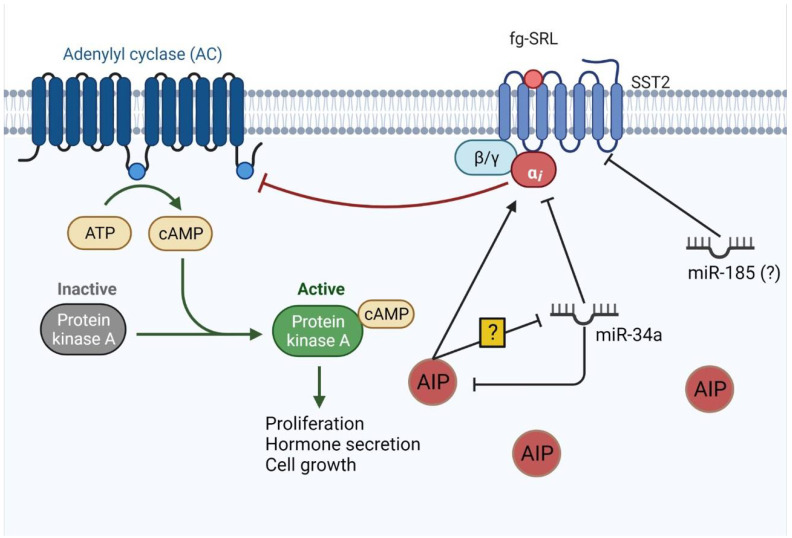
Acromegaly is a chronic and systemic disease due to excessive growth hormone and insulin-like growth factor type I caused, in the vast majority of cases, by a GH-secreting pituitary adenoma. About 40% of these tumors have somatic mutations in the stimulatory G protein alpha-subunit 1 gene. The pathogenesis of the remaining tumors, however, is still not fully comprehended. Surgery is the first-line therapy for these tumors, and first-generation somatostatin receptor ligands (fg-SRL) are the most prescribed medications in patients who are not cured by surgery. MicroRNAs are small, non-coding RNAs that control the translation of many mRNAs, and are involved in the post-transcriptional regulation of gene expression. Differentially expressed miRNAs can explain differences in the pathogenesis of acromegaly and tumor resistance. In this review, we focus on the most validated miRNAs, which are mainly involved in acromegaly’s tumorigenesis and fg-SRL resistance, as well as in circulating miRNAs in acromegaly.
Keywords: acromegaly; miRNA; somatostatin receptor ligands; tumorigenesis.
Conflict of interest statement
M.R.G. has served as an advisory board member for Ipsen, Novartis Pharmaceuticals, Novo Nordisk, Recordati Rare Diseases, and Crinetics Pharmaceuticals; as a research investigator for Crinetics Pharmaceuticals, Recordati Rare Diseases, and Novartis Pharmaceuticals; and as a speaker for Crinetics Pharmaceuticals, Novartis Pharmaceuticals, Ipsen, Novo Nordisk, and Recordati Rare Diseases. L.K. has received speaker fees from Novartis and Ipsen.
Figures
Similar articles
-
miR-383-5p, miR-181a-5p, and miR-181b-5p as Predictors of Response to First-Generation Somatostatin Receptor Ligands in Acromegaly.Int J Mol Sci. 2023 Feb 2;24(3):2875. doi: 10.3390/ijms24032875. Int J Mol Sci. 2023. PMID: 36769196 Free PMC article.
-
Survivin: A Potential Marker of Resistance to Somatostatin Receptor Ligands.J Clin Endocrinol Metab. 2023 Mar 10;108(4):876-887. doi: 10.1210/clinem/dgac610. J Clin Endocrinol Metab. 2023. PMID: 36273993
-
Somatostatin receptor expression and patients' response to targeted medical treatment in pituitary tumors: evidences and controversies.J Endocrinol Invest. 2020 Nov;43(11):1543-1553. doi: 10.1007/s40618-020-01335-0. Epub 2020 Jun 18. J Endocrinol Invest. 2020. PMID: 32557353 Review.
-
Somatostatin Receptor Expression in GH-Secreting Pituitary Adenomas Treated with Long-Acting Somatostatin Analogues in Combination with Pegvisomant.Neuroendocrinology. 2017;105(1):44-53. doi: 10.1159/000448429. Epub 2016 Jul 25. Neuroendocrinology. 2017. PMID: 27455094 Free PMC article.
-
Pasireotide in the Personalized Treatment of Acromegaly.Front Endocrinol (Lausanne). 2021 Mar 16;12:648411. doi: 10.3389/fendo.2021.648411. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 33796079 Free PMC article. Review.
Cited by
-
Delving into Acromegaly.J Clin Med. 2023 Feb 19;12(4):1654. doi: 10.3390/jcm12041654. J Clin Med. 2023. PMID: 36836189 Free PMC article.
-
The clinical effects of miR-26a, miR-16, let-7, miR-128a and miR-223 in acromegaly.Ir J Med Sci. 2025 Aug 11. doi: 10.1007/s11845-025-04068-2. Online ahead of print. Ir J Med Sci. 2025. PMID: 40788444
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
