

Recovering or Persisting: The Immunopathological Features of SARS-CoV-2 Infection in Children
- PMID: 35955979
- PMCID: PMC9369242
- DOI: 10.3390/jcm11154363
Recovering or Persisting: The Immunopathological Features of SARS-CoV-2 Infection in Children
Abstract
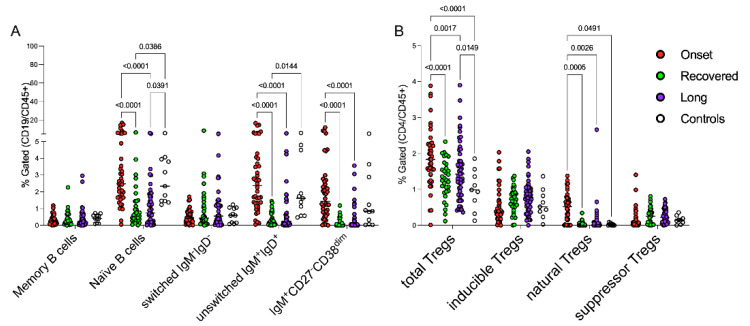
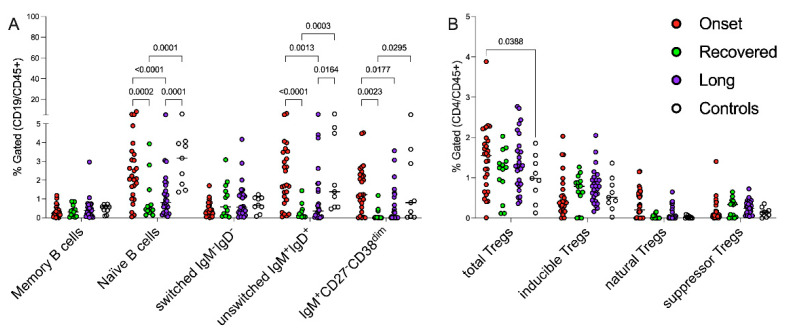
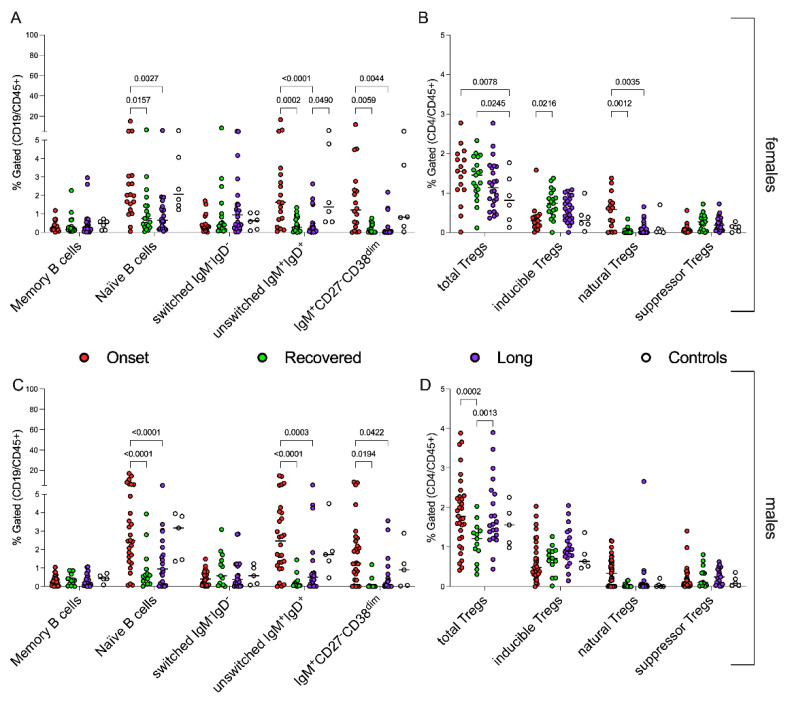
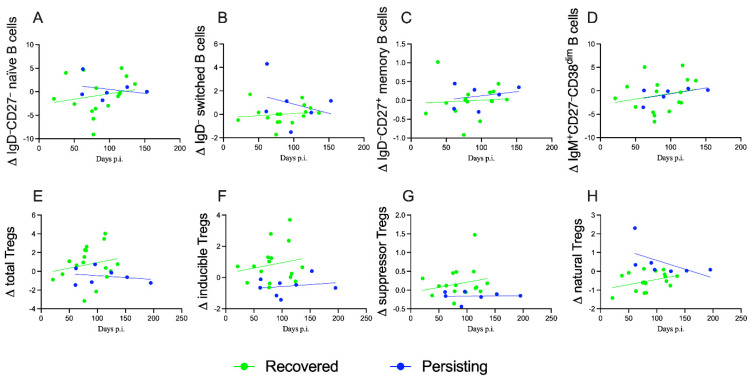
Background. The profile of cellular immunological responses of children across the spectrum of COVID-19, ranging from acute SARS-CoV-2 infection to full recovery or Long COVID, has not yet been fully investigated. Methods. We examined and compared cytokines in sera and cell subsets in peripheral blood mononuclear cells (B and regulatory T lymphocytes) collected from four distinct groups of children, distributed as follows: younger than 18 years of age with either acute SARS-CoV-2 infection (n = 49); fully recovered from COVID-19 (n = 32); with persistent symptoms (Long COVID, n = 51); and healthy controls (n = 9). Results. In the later stages after SARS-CoV-2 infection, the cohorts of children, both with recovered and persistent symptoms, showed skewed T and B subsets, with remarkable differences when compared with children at the onset of the infection and with controls. The frequencies of IgD+CD27− naïve B cells, IgD+IgM+ and CD27−IgM+CD38dim B cells were higher in children with recent infection than in those with an older history of disease (p < 0.0001 for all); similarly, the total and natural Tregs compartments were more represented in children at onset when compared with Long COVID (p < 0.0001 and p = 0.0005, respectively). Despite the heterogeneity, partially due to age, sex and infection incidence, the susceptibility of certain children to develop persistent symptoms after infection appeared to be associated with the imbalance of the adaptive immune response. Following up and comparing recovered versus Long COVID patients, we analyzed the role of circulating naïve and switched B and regulatory T lymphocytes in counteracting the evolution of the symptomatology emerged, finding an interesting correlation between the amount and ability to reconstitute the natural Tregs component with the persistence of symptoms (linear regression, p = 0.0026). Conclusions. In this study, we suggest that children affected by Long COVID may have a compromised ability to switch from the innate to the adaptive immune response, as supported by our data showing a contraction of naïve and switched B cell compartment and an unstable balance of regulatory T lymphocytes occurring in these children. However, further prospective immunological studies are needed to better clarify which factors (epigenetic, diet, environment, etc.) are involved in the impairment of the immunological mechanisms in the Long COVID patients.
Keywords: COVID-19 immunopathology; T cells; childhood SARS-CoV-2 infection; pediatric Long COVID.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Götzinger F., Santiago-García B., Noguera-Julián A., Lanaspa M., Lancella L., Carducci F.I.C., Gabrovska N., Velizarova S., Prunk P., Osterman V., et al. COVID-19 in Children and Adolescents in Europe: A Multinational, Multicentre Cohort Study. Lancet Child Adolesc. Health. 2020;4:653–661. doi: 10.1016/S2352-4642(20)30177-2. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
